Background: Deep sedation has been shown to be safe and feasible for the pentaspline (ps) PFA system. Skeletal muscle, phrenic nerve stimulation, and esophageal contraction have caused discussions about sedation protocols when PFA is performed in deep sedation, but data remain scarce.
Objective: To compare the doses of sedation and analgesia and evaluate safety of deep sedation during index PVI using cryoballoon (CB) and psPFA.
Methods: Patients undergoing index PVI were consecutively enrolled into TRUST, a prospective, single-center, clinical cohort study (NCT05521451). Sedation was initiated using a bolus of 0.5mg/kg propofol and 25µg fentanyl, and maintained using continuous propofol administration at 6-7mg/(kg*min). Additional boluses or higher propofol rates were applied at the discretion of the operator when sedation depth or analgesia were deemed insufficient. To account for procedure time and patient weight, propofol and fentanyl doses were indexed to both of these parameters (mg/(kg*min); ng/(kg*min)).
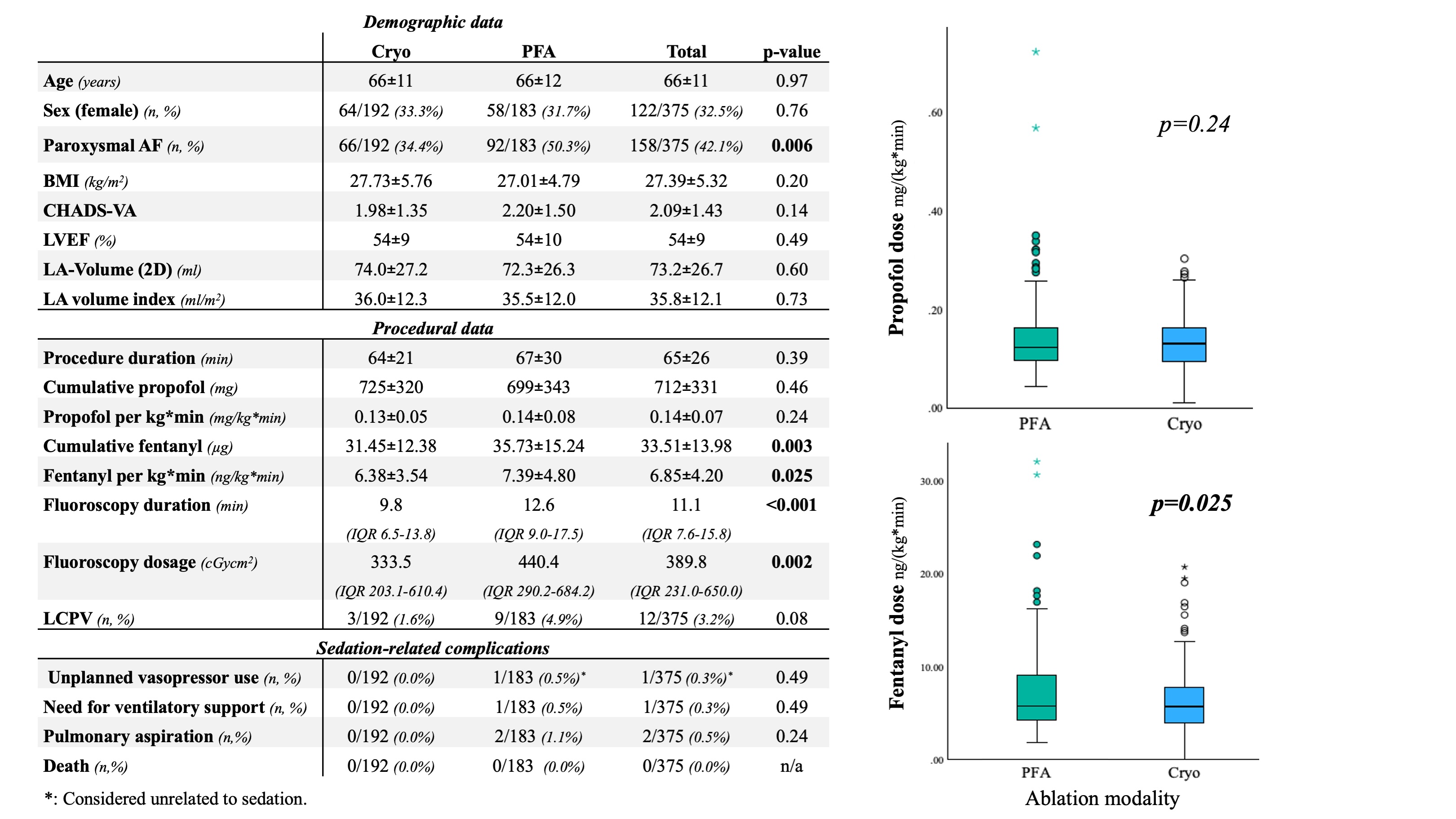
Results: In total, 375 patients (192 CB, 183 psPFA) were included. Patient characteristics are displayed in the Figure. In the psPFA group, fentanyl doses were significantly higher than in the CB group (7.39±4.80 ng/(kg*min) vs. 6.38±3.54 ng/(kg*min); p=0.025). There was no difference in propofol doses between the groups (0.14±0.08 mg/(kg*min) vs. 0.13±0.05 mg/(kg*min); p=0.24). Sedation-related adverse events were rare: Intraprocedural pulmonary aspiration occurred in 2/183 patients (1.1%) from the psPFA group, one of which required intermittent bag ventilation (1/183; 0.5%). Both patients were treated with antibiotics prophylactically and did not develop pneumonia. In both cases, the hospital stay was not prolonged due to pulmonary aspiration. No sedation-related complications occurred in the CB-group.
Conclusion: Pulsed-field ablation with deep sedation is safe and feasible in this series. Higher opioid doses during psPFA procedures suggest an increased need for analgesia, potentially to mitigate pain from energy delivery or skeletal muscle activation. Monitoring for signs of intraprocedural pulmonary aspiration during PFA procedures could further reduce sedation-related risks during PFA ablation.
Figure: