Background: Atrial tachycardias (AT) are increasingly encountered in clinical practice. While rhythm control is effective and guideline-endorsed, evidence on long-term outcomes is lacking.
Aim: Here, we aimed to evaluate long-term outcomes following initial AT catheter ablation vs. electrocardioversion.
Methods: The present multicentre observational registry enrolled consecutive patients undergoing AT rhythm control. The composite primary endpoint including mortality, stroke and cardiovascular hospitalization and its individual components were assessed and compared between catheter ablation vs. electrocardioversion using all-comers and propensity score-matched analyses.
Results: Among 1115 patients (64.9±14.1 years, 55.6% male), the majority underwent catheter ablation as the primary treatment strategy (95.0%). During a follow-up of 2478 patient-years, the composite primary endpoint occurred less frequently after catheter ablation compared with electrocardioversion (28.03 vs. 45.14 events/100 patient-years; HR 0.37; 95% CI 0.23–0.60; P<0.0001) (Figure), and the time until the first event was longer (8.6 [IQR 3.7–22.1] months vs. 2.8 [IQR 1.4–8.5] months; P<0.0001), even after propensity score-matching. Predictors of the composite primary endpoint included age, AT history, the CHA2DS2-VA score, cardiovascular comorbidities such as atrial fibrillation and arterial hypertension, previous atrial ablation, and procedural characteristics like reentrant AT ablation (P<0.01 each). All-cause mortality (1.22 vs. 5.39 events/100 patient-years; HR 0.23; 95% CI 0.01–3.93; P=0.0273), cardiovascular mortality (0.21 vs. 2.69 events/100 patient-years; HR 0.09; 95% CI 0.01–36.55; P=0.0067) and the incidence of stroke within the first 6 months following AT rhythm control (0.04 vs. 1.0 events/100 patient-years; HR 0.05; 95% CI 0–39.58; P=0.0017) were reduced after ablation vs. electrocardioversion. Cardiovascular hospitalization was less often required after catheter ablation (27.48 vs. 45.14 events/100 patient-years; HR 0.37; 95% CI 0.23–0.60; P<0.0001), with a longer time until first hospitalization (8.4 [IQR 3.6–21.8] months vs. 2.8 [IQR 1.4–8.5] months; P<0.0001).
Conclusions: This large multicentre registry suggests that catheter ablation as the predominant AT rhythm control strategy is associated with lower risks of mortality, stroke and cardiovascular hospitalization compared with electrocardioversion, supporting a reassuring safety profile and sustained prognostic benefit, even among patients with multiple cardiovascular comorbidities.
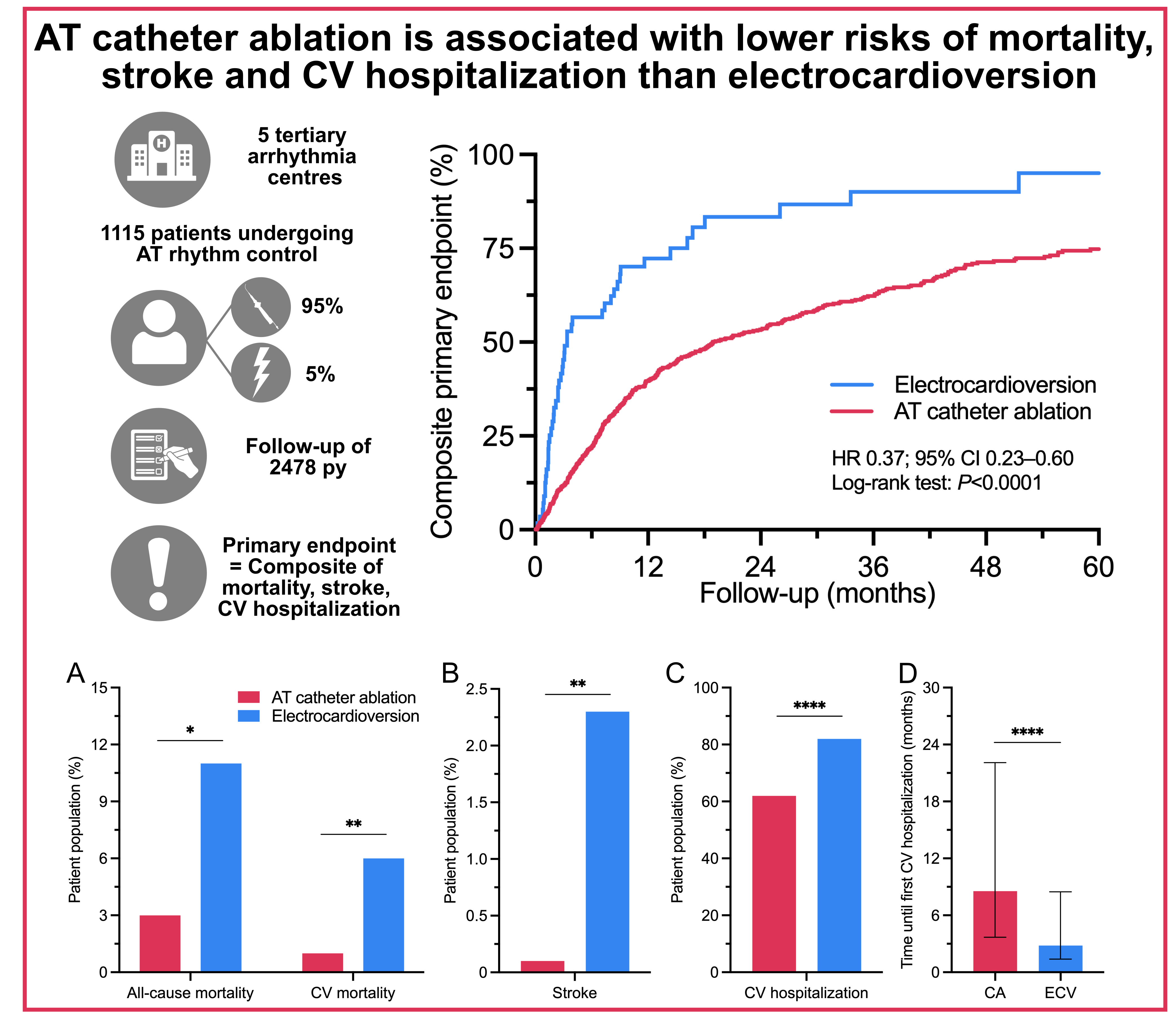
Figure. Reduced mortality, strokes and CV hospitalizations after initial AT catheter ablation vs. electrocardioversion.
AT catheter ablation is associated with lower risks of A, mortality, B, stroke at 6 months following AT rhythm control and C, CV hospitalization and D, a longer time until first CV hospitalization compared with electrocardioversion. CA = catheter ablation; CV = cardiovascular; ECV = electrocardioversion. **** P<0.0001; ** P<0.01; * P<0.05.



