Background: The growing prevalence of atrial tachycardias (AT) represents an increasingly relevant clinical challenge, with major impact on patients and healthcare systems. While rhythm control has emerged as the treatment of choice, subsequent cardiovascular hospitalizations in these patients have not been systematically assessed yet.
Methods: The present multicentre observational registry included consecutive patients undergoing AT rhythm control defined as catheter ablation or electrocardioversion. Prevalence, reasons and predictors of cardiovascular hospitalizations during a follow-up of 2.2±2.6 years were assessed.
Results: Among 1115 patients (64.9±14.1 years, 55.6% male, previous cardiac intervention in 76.8%), 699 (62.7%) were hospitalized for cardiovascular reasons after initial AT rhythm control. The first hospitalization was required after 7.8 [IQR 3.2–18.9] months (range 2–5526 days), predominantly due to arrhythmia recurrence (85.7%). Univariate predictors of cardiovascular hospitalization were an increased age (HR 1.05; 95% CI 1.01–1.08; P=0.0051), body mass index (HR 1.03; 95% CI 1.01–1.05; P=0.0022) and CHA2DS2-VA score (HR 1.10; 95% CI 1.04–1.17; P=0.0013), a reduced left ventricular ejection fraction (HR 0.95; 95% CI 0.91–0.99; P=0.0226) and AT cycle length (HR 0.986; 95% CI 0.974–0.998; P=0.0215) and concomitant atrial fibrillation (HR 1.55; 95% CI 1.27–1.91; P<0.0001). Ablation of ≥1 reentrant AT (HR 1.63; 95% CI 1.24–2.17; P=0.0003) or reentrant AT only (HR 1.81; 95% CI 1.40–2.36; P<0.0001) was associated with cardiovascular hospitalization, whereas ablation of non-reentrant AT only was not (HR 0.60; 95% CI 0.45–0.79; P=0.0002) (Figure). In multivariate analysis, a reduced left ventricular ejection fraction and reentrant AT ablation remained significant predictors of cardiovascular hospitalization.
Conclusions: This large multicentre registry indicates that cardiovascular hospitalizations are required in two-thirds of patients undergoing AT rhythm control, predominantly due to arrhythmia recurrence. The higher prevalence of cardiovascular comorbidities among hospitalized patients underscores the importance of structured risk factor modification as an essential part of long-term arrhythmia management to reduce healthcare burden after AT rhythm control.
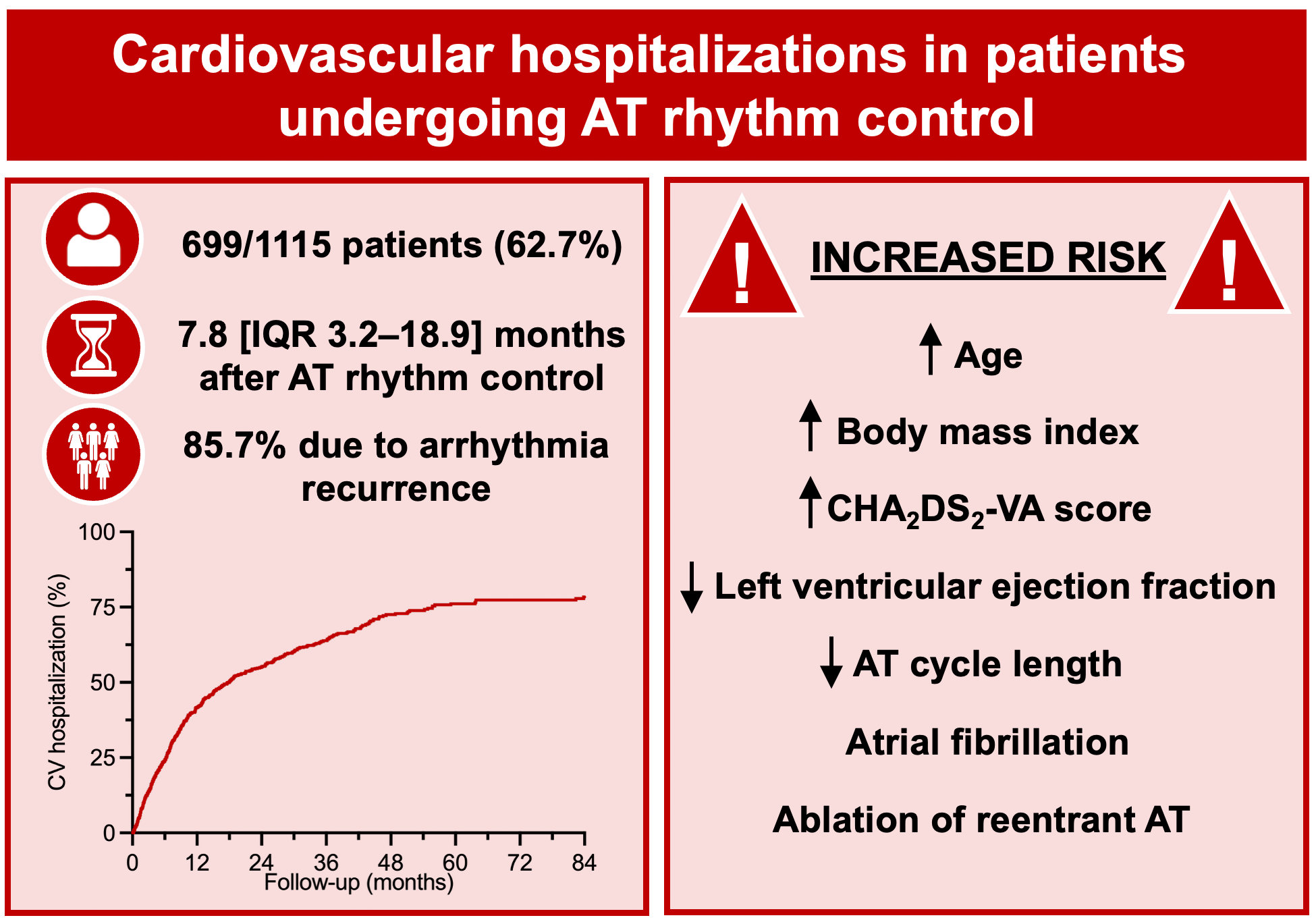
Figure. CV hospitalizations in patients undergoing AT rhythm control.
CV hospitalizations are required in two-thirds of patients undergoing AT rhythm control, predominantly due to arrhythmia recurrence and occurring within the first year. Predictors include clinical and procedural characteristics. CV = cardiovascular.



