Background: Autonomic innervation and inflammation play a pivotal role in the initiation and maintenance of atrial fibrillation (AF). Pulmonary vein isolation (PVI) alters not only myocardial electrophysiological properties but also autonomic pathways and already ongoing inflammatory processes in the atria, which may affect long-term rhythm stabilization.
Aim: Therefore, we aimed to characterize post-ablation autonomic remodeling and inflammatory response in relation to rhythm outcome in patients with AF.
Methods: Thirty patients (63 [IQR 53–68] years, 60% male) undergoing cryoballoon PVI for paroxysmal AF were prospectively included. Blood parameters were measured before, 1 day after, and 3 months after PVI. Heart rate variability was assessed before and 3 months after PVI. Results were compared between patients with (n=14) and without AF recurrence (n=16) during the first 3 months, as determined by mobile electrocardiograms recorded by the patients twice daily and during symptoms.
Results: Both, patients in sinus rhythm (SR) and those with AF recurrence, exhibited a transient post-procedural rise in IL-6 followed by a decline at 3 months (P<0.01 each). In contrast, adiponectin, an anti-inflammatory and cardioprotective adipokine, decreased (37.2 [IQR 25.3–68.4] µg/ml vs. 36.0 [IQR 21.7–68.7] µg/ml; P=0.0098) and β-NGF, indicating neural regeneration, increased after PVI (3.6 [IQR 2.7–4.1] µg/ml vs. 3.6 [IQR 3.2–4.4] µg/ml; P=0.0156) only in SR patients, whereas none of these effects were observed in patients with AF recurrence. Three months after PVI, patients maintaining SR presented with enhanced sympathetic (stress index: 8.5 [IQR 5.6–22.0] ms vs. 25.6 [IQR 10.7–29.6] ms; P=0.0156) and reduced parasympathetic activity, reflected by lower RMSSD (43.0 [IQR 14.6–85.2] ms vs. 14.8 [IQR 10.1–35.6] ms; P=0.0078), pNN50 (1.8 [IQR 1.5–2.1] ms vs. 1.4 [IQR 1.2–1.6] ms; P=0.0234) and HF (426.0 [IQR 41.0–2957.0] ms2 vs. 67.0 [IQR 40.0–373.5] ms2; P=0.0156) (Figure). Only SR patients showed an increase in SDNN (11.9 [IQR 8.4–33.5] ms vs. 24.7 [IQR 11.1–37.6] ms; P=0.0061) and LF/HF (0.8 [IQR 0.3–1.6] ms2/ms2 vs. 2.1 [IQR 0.6–9.6] ms2/ms2; P=0.0398) under respiratory modulation, indicating sympathetic-parasympathetic balance, while no autonomic changes were observed in patients with AF recurrence.
Conclusion: After PVI, a transient inflammatory response is observed in all patients, while a concurrent adiponectin decrease in those maintaining SR may reflect metabolic-inflammatory normalization. Increased β-NGF and heart rate variability changes consistent with autonomic reorganization in SR patients suggest favorable neural remodeling associated with successful rhythm stabilization.
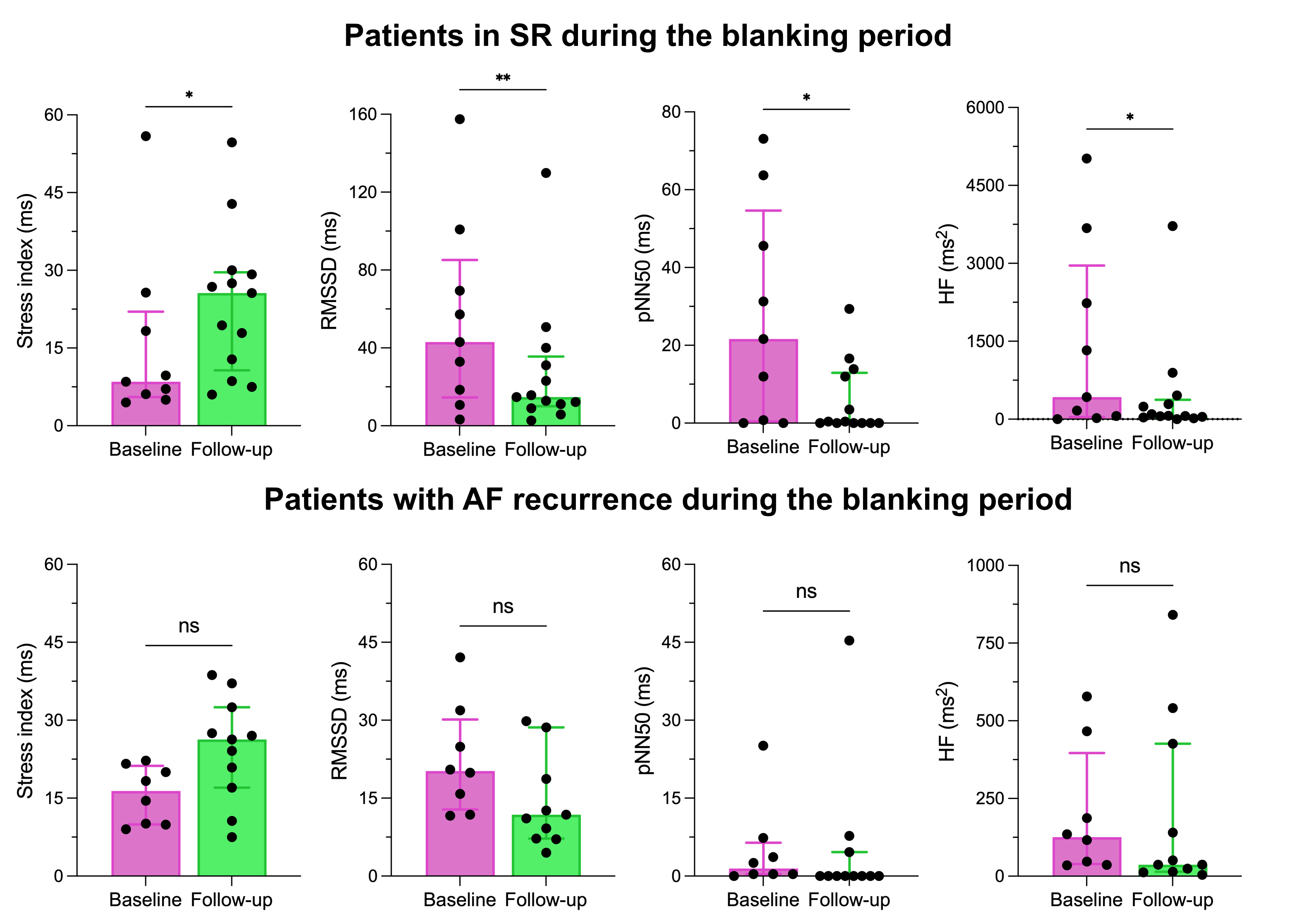
Figure. Autonomic remodeling after PVI. ** P<0.01; * P<0.05.



