Background: The 2023 ESC guidelines for the management of ACS recommend an assessment of patients with acute chest pain via electrocardiogram (ECG) and serial troponin assessment, classifying patients into rule-in, rule-out or into a group with further testing and observation recommended. We aimed to evaluate, whether an initial point-of-care echocardiography evaluation can improve the prediction of obstructive coronary artery disease (CAD) above initial ECG and troponin evaluation alone. Methods: The present analysis is based on the prospective EPIC-ACS study (Epicardial adipose tissue thickness predicts obstructive coronary artery disease in ACS patients) of patients presenting with acute chest pain, suggestive of ACS, to the emergency department of the University Hospital Essen. Patients with STEMI, haemodynamic instability or known CAD were excluded. Patients with suspected ACS were examined by a blinded echocardiographer. The following characteristics were assessed: normal vs. impaired left ventricular ejection fraction (LVEF, ≥50% or <50%), presence of regional wall motion abnormalities (RWMA, yes or no), the left-atrial diameter in parasternal long axis view, and an epicardial adipose tissue (EAT) thickness of < vs. ≥5.5mm. The primary endpoint was defined as the presence of obstructive CAD detected in subsequent invasive coronary angiography. Results: Between 2019 and 2020, a total of 511 (Age: 57.52±18.1 years, 52% male) patients were included in this prospective observational cohort study. Of these 511 patients, 214 were transferred to invasive coronary angiography, of which 97 patients had obstructive CAD. Comparing the echocardiographic parameters of the patients with obstructive CAD, independent of the ACS-pathway, patients with obstructive CAD had significantly more often RWMA (26.8% vs. 6.1%, p<0.001) and significantly more often an EAT of ≥5.5mm (88.7% vs. 11.3%, p<0.001). LVEF group and left-atrial diameter were not significantly different between patients with vs. without obstructive CAD (LVEF≥50%: 81.4% vs. 87.7%, p=0.48, LA-Diameter >4.5cm: 5.2% vs. 6.3%, p=0.44). Figure 1 shows the presence of obstructive CAD, stratified by echocardiographic parameters with normal and abnormal values showing that EAT ≥5.5mm was markedly more frequently presence in patients with obstructive CAD (p<0.001, over all three pathways). In addition, the presence of RWMA differentiated patients with and without obstructive CAD in the rule-in pathway (76% vs. 40%, p=0.003) and rule-out pathway (26% vs. 6%, p=0.028), while no significant difference was observed for the observe group (p=0.173). LVEF (rule-in: p=0.313, observe: p=0.441, rule-out: p=0.685) and LA-Diameter (rule-in: p=0.084, observe: p=0.832, rule-out: p=0.531) did not qualify for differentiating patients with and without obstructive CAD.
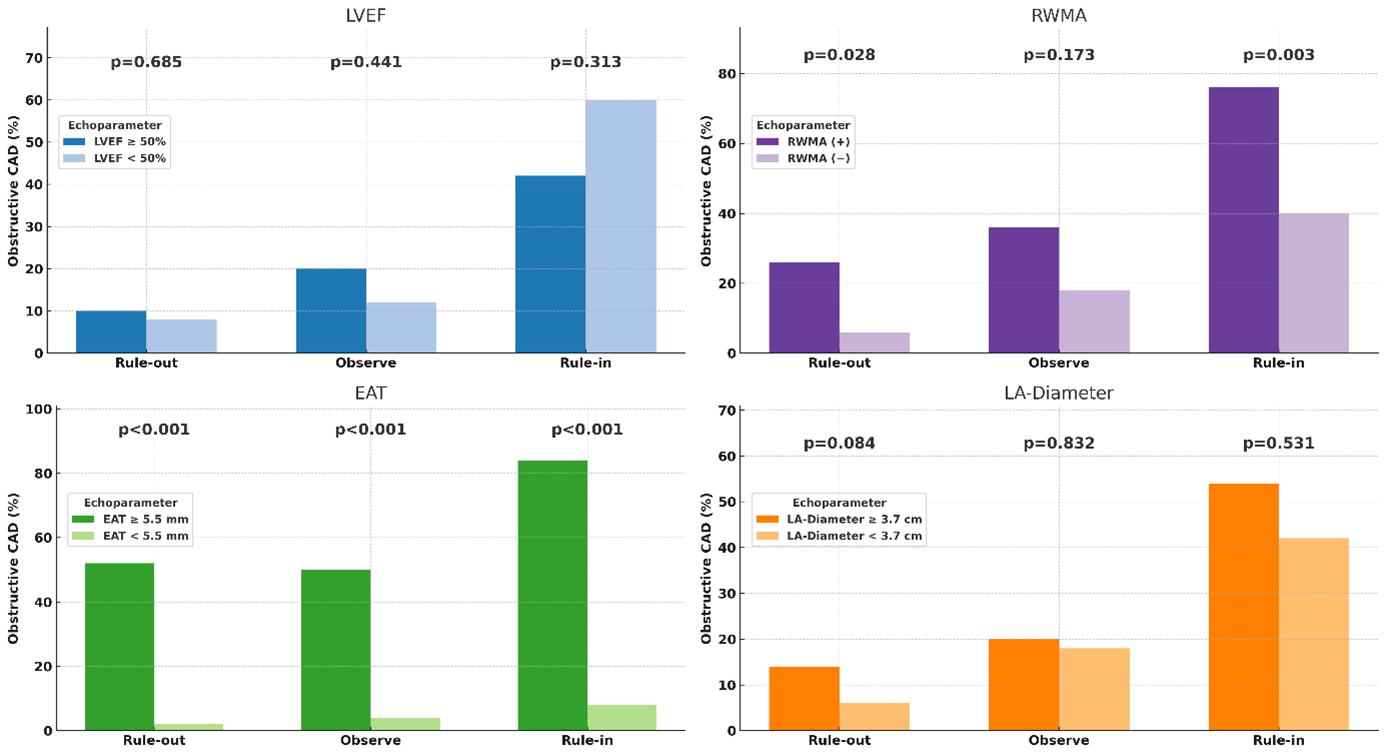
Figure 1: Frequency of obstructive CAD in patients with LVEF < vs. ≥50%, presence vs. absence of RWMA, EAT thickness of < vs. ≥5.5 mm, and LA diameter < vs. ≥median, stratified by the guideline-recommended pathway into rule-out, observe or rule-in. Conclusion: Point-of-care echocardiography can help to re-stratify patients with acute chest pain in addition to the guideline-recommended rule-in or rule-out pathway. Our results support the frequent use of point-of-care echocardiographyfor clinical decision-making in patients suspected ACS.



