Introduction:
Left bundle branch area pacing (LBBAP) is a promising alternative to right ventricular pacing with a growing body of evidence. It is unclear whether the AV-delay should be shortened, prolonged or maintained the same during pacing with a higher heart rate. Therefore, we aimed to compare the acute hemodynamic effects of different AV-delays while pacing with different heart rates.
Methods:
Recipients of LBBAP with intrinsic rhythm <60 bpm and who had no intrinsic conduction under atrial pacing were consecutively enrolled. Left ventricular outflow tract velocity time integral (LVOT-VTI) and left ventricular filling time (LVFT) were measured at 60, 80 and 100 bpm. For every heart rate, measurements were performed five times at random order - with the prespecified AV-delay (60 bpm: 180ms, 80 bpm: 160ms, 100 bpm: 140ms), as well as 40 and 80 ms shortened and prolonged using DDD-pacing. Echocardiography was performed using a GE Healthcare, Vivid E95 system after 30 seconds of an establishment phase. The echocardiographer was blinded towards the AV-delay settings.
Results:
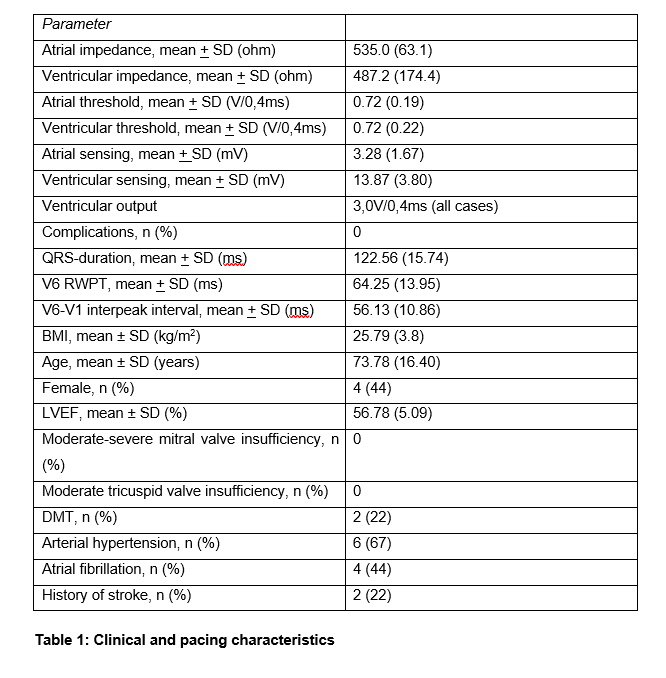
9 patients with BIOTRONIK Enitra 6 DR pacemakers were included. Clinical and echocardiographic characteristics are summarized in table 1. LBBAP (Left bundle branch pacing (LBBP), left bundle fascicular pacing (LBFP) and left ventricular septal pacing (LVSP)) was defined according to the 2023 EHRA consensus statement and was demonstrated in all patients at the time of measurement (see table 2).
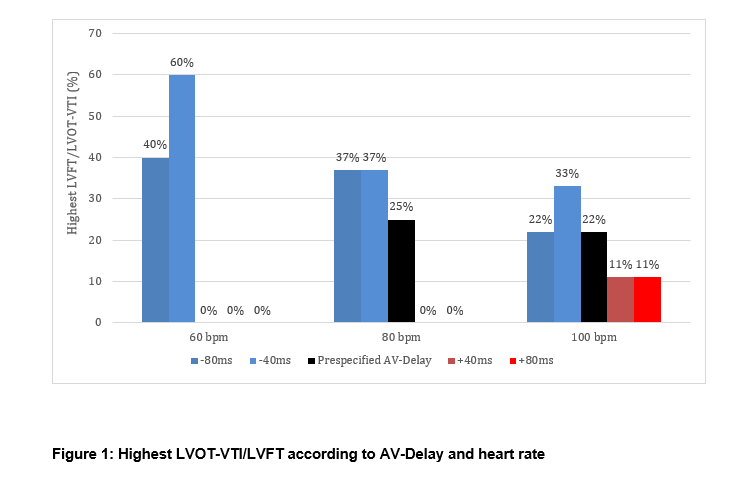
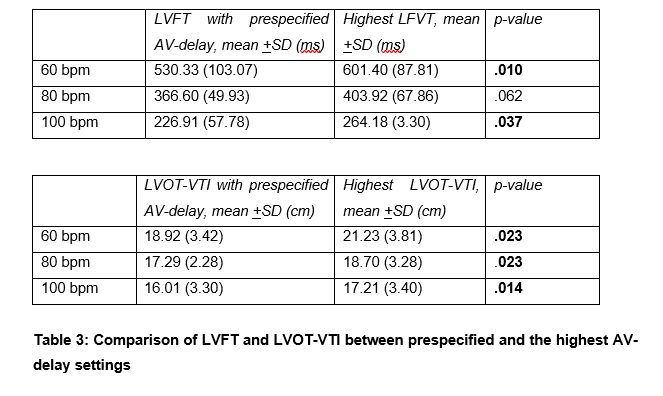
The optimal AV delay varied widely between patients and heart rates. In some cases, the hemodynamically optimal delay was shorter, in others longer than the prespecified value (see figure 1). The prespecified AV-delay was associated with the highest LVOT-VTI/LVFT at 60 bpm in 0%, at 80 bpm in 25% and at 100 bpm in 22% (see figure 1). Individualized AV delay increased LVOT-VTI by 8-12% and LVFT by 10–14% across the tested heart rates, with statistically significant improvements for most comparisons (see table 3).
Conclusion:
In this pilot study, a prespecified AV-delay in LBBAP was rarely associated with the best hemodynamic status. Individualized programming of the AV-delay significantly improved hemodynamics in most cases. These results challenge the notion of using a prespecified AV-delay in LBBAP and underline the necessity for individualized programming.