Background
Transcatheter tricuspid interventions are promising for severe TR, yet patient selection remains difficult, as many present too late. NT-proBNP has limited prognostic value. Growth differentiation factor-15 (GDF-15) and soluble urokinase plasminogen activator receptor (suPAR) reflect inflammation, oxidative stress, and organ dysfunction, potentially capturing disease burden beyond haemodynamics. Elevated right atrial (RA) pressure signals poor outcomes, but its added value to biomarker-based prediction is unclear. This study assessed whether GDF-15 and suPAR predict 1-year mortality after transcatheter tricuspid intervention and whether adding RA pressure improves risk stratification.
Methods
In a prospective single-centre cohort, we analysed patients undergoing transcatheter tricuspid intervention including T-TEER (TriClip, Pascal) and heterotopic/orthotopic valve systems (TricValve, Evoque). Blood sampling was performed before intervention. NT-proBNP was measured in routine diagnostics; GDF-15 and suPAR via ELISA. All patients underwent pre-interventional right-heart catheterization to record RA pressure. Receiver operating characteristic (ROC) analyses with area under the curve (AUC) quantified predictive performance for 1-year mortality. Models combining biomarkers with RA pressure assessed incremental value. Optimal biomarker cut-offs were defined by the Youden index. AUC 0.60–0.69 was considered poor, 0.70–0.79 fair, 0.80–0.89 good, and 0.90–1.00 excellent.
Results
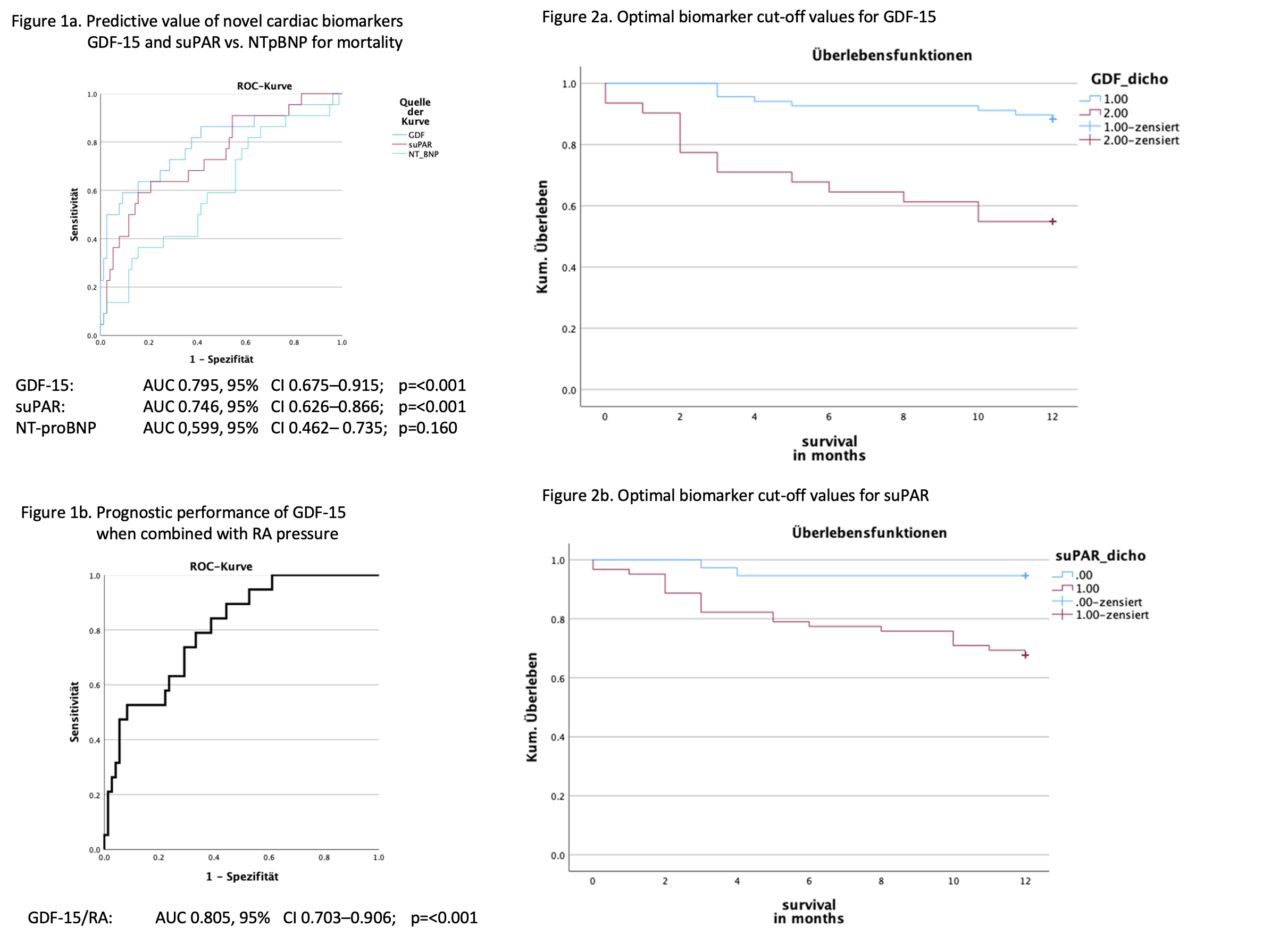
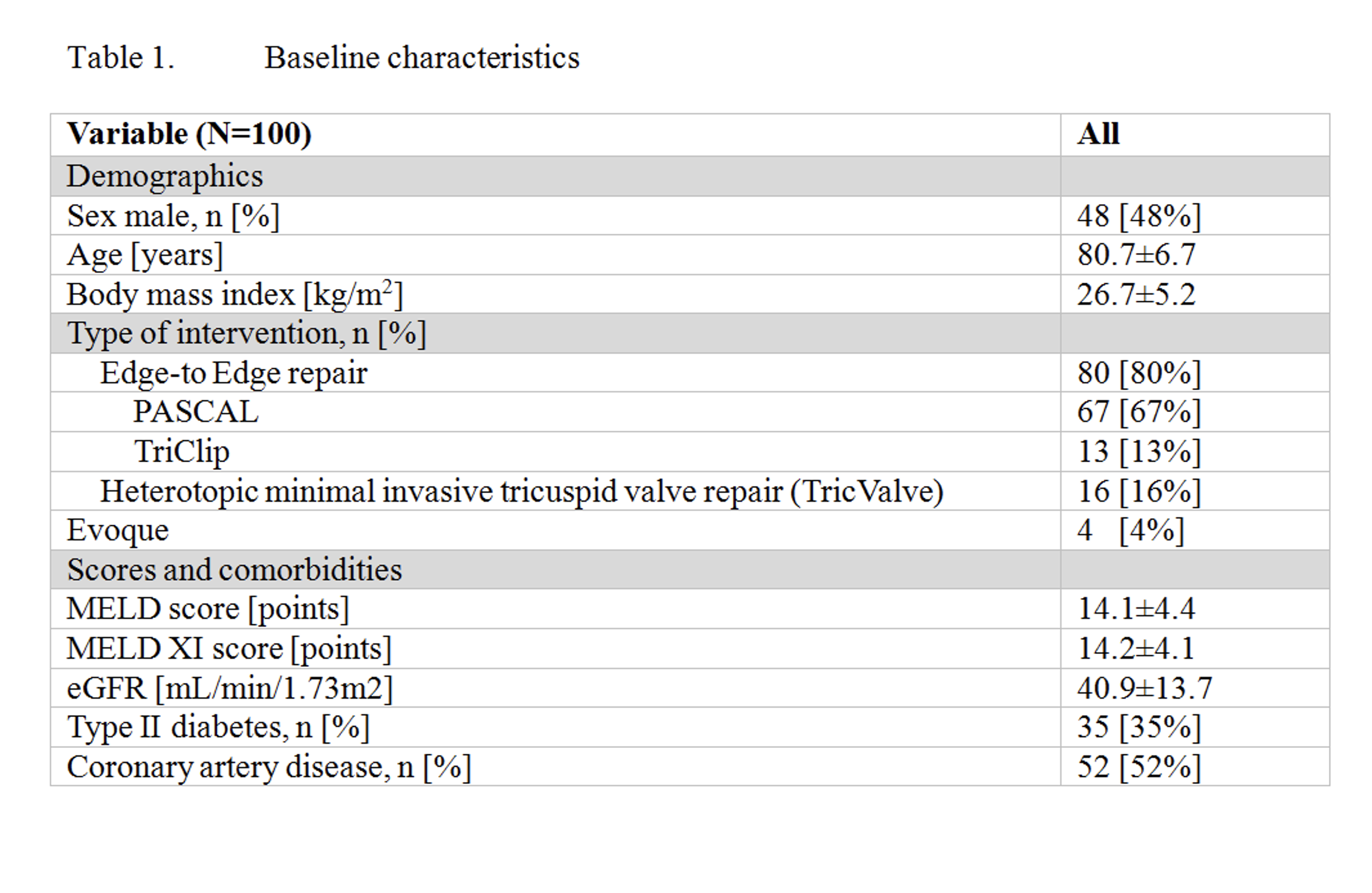
We analysed 100 consecutive patients (age 80.7±6.7 years, 48% male, MELD 14.02±4.41). T-TEER was performed in 80 patients (TriClip n=13; Pascal n=67); 20 received valve systems (TricValve n=16; Evoque n=4). Within 1 year, 22 patients (22%) died. GDF-15 showed the highest predictive accuracy (AUC 0.795; 95% CI 0.675–0.915; p<0.001), followed by suPAR (AUC 0.746; 95% CI 0.626–0.866; p<0.001). Both outperformed NT-proBNP (AUC 0.599; 95% CI 0.462–0.735; p=0.160) Figure 1a. Combining GDF-15 with RA pressure improved discrimination (AUC 0.805; 95% CI 0.703–0.906; p<0.001), indicating incremental prognostic value Figure 1b. The optimal GDF-15 cut-off was 2,400 pg/mL, identifying patients with lower 1-year survival (log-rank χ²=16.269; p<0.001) Figure 2a. For suPAR, the optimal cut-off was 3,350 pg/mL, also associated with impaired survival (log-rank χ²=9.239; p=0.002) Figure2b.
Conclusion
GDF-15 and suPAR outperformed NT-proBNP in predicting 1-year mortality after transcatheter tricuspid intervention. Elevated values indicate high-risk patients, and integrating RA pressure further refines risk assessment, supporting improved timing and selection for intervention.