Introduction:
Left atrial appendage (LAA ) thrombus formation is a known complication of atrial fibrillation that may occur despite adequate oral anticoagulation (OAC) and is associated with elevated stroke risk and mortality. However, data on the anticoagulation strategy associated with the highest resultion rate is lacking. Therefore, we compared different therapeutic strategies in patients presenting with LAA thrombi under OAC therapy.
Methods:
In this retrospective single-center study, 216 patients with atrial fibrillation and LAA thrombus despite OAC for more than three weeks were identified. Follow-up transesophageal echo (TEE) performed after a period of at least four weeks and was available for all patients. Clinical and echocardiographic parameters as well as anticoagulation regimen were compared between patients with and without thrombus resolution.
Results:
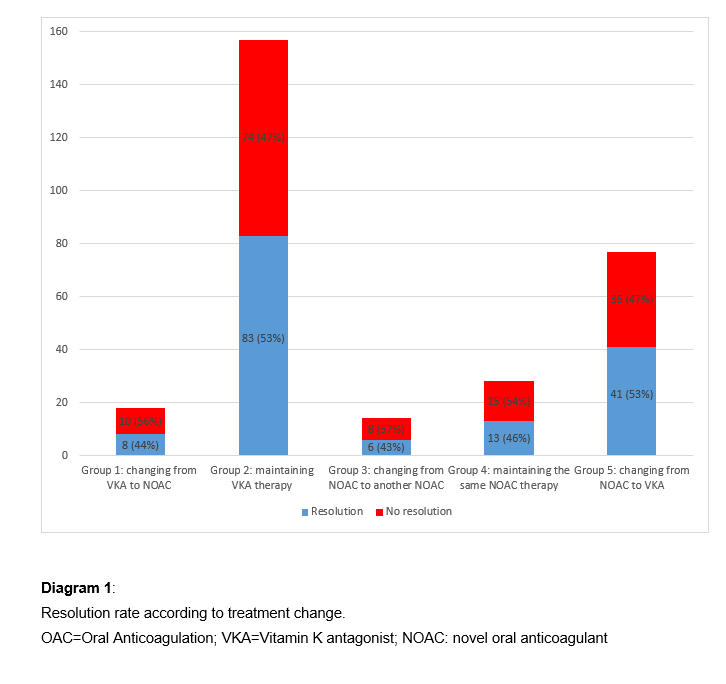
Median age was 72 years (IQR 13), CHADS-Vasc score was elevated at 4 (IQR 2). Some patients consecutively underwent different treatment cycles. Each treatment cycle was analyzed, five treatment strategies were identified:
Group 1 (Changing from VKA to NOAC),
Group 2 (Maintaining VKA therapy with enhanced adherence/time in therapeutic range),
Group 3 (Changing from NOAC to another NOAC),
Group 4 (Maintaining the same NOAC therapy) and
Group 5 (Changing from NOAC to VKA).
216 patients were included with 294 treatment cycles. The resolution rate was 51% (151/294) after a median treatment cycle duration of 61.5 days (IQR 50).
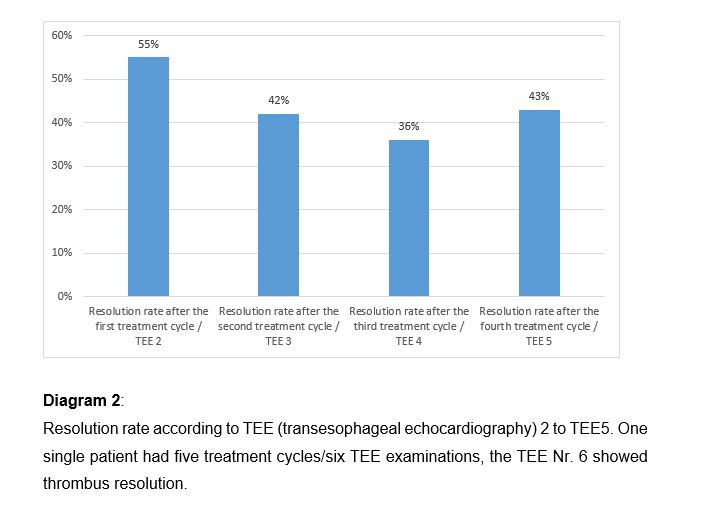
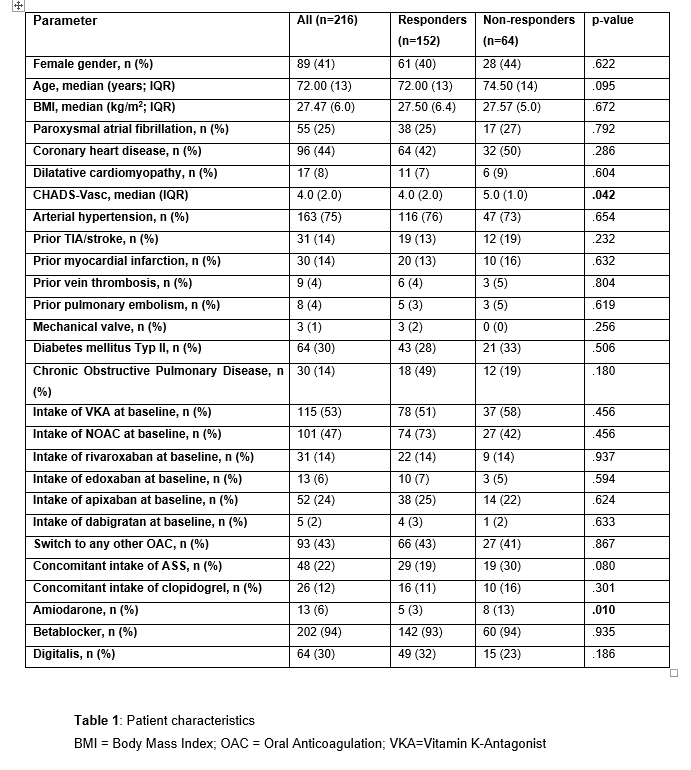
Patients without thrombus resolution had higher CHADS-Vasc-Score and took amiodaron more frequently (see table 1). However, multivariate regression analysis identified no parameters predictive of LAA thrombus resolution. No statistical difference in resolution rate between the five anticoagulation strategies was observed (p=0.866, see diagram 1). After the first treatment cycle/second TEE, the resolution rate was highest at 55% and declined thereafter (see diagram 2).
Conclusion:
This is the largest cohort of patients presenting with LAA thrombus despite ongoing OAC.
Since no anticoagulation regimen proved superior, continuing the existing OAC appears to be a reasonable approach.