Background
Chronic kidney disease (CKD) is a major determinant of disease progression in heart failure with preserved ejection fraction (HFpEF). Cardiorenal interaction accelerates symptom progression and increases mortality. Early identification of patients at risk for renal deterioration before overt HFpEF develops is therefore crucial. Urinary Dickkopf-3 (uDKK3), a stress-induced glycoprotein secreted by renal tubular cells, has been shown to predict future decline in renal function. We hypothesized that uDKK3 enables early identification of patients with incipient HFpEF at risk for subsequent renal impairment.
Methods
Between 02/24 and 11/24, we prospectively recruited 99patients at risk for HFpEF (AHA Stage A/B) from Nephrology and Cardiology outpatient departments at the University Medical Center Göttingen during routine appointments unrelated to heart failure.
Patients were included if they had ≥1HFpEF risk factor (age >60 years, arterial hypertension, diabetes mellitus, CKD, obesity, or a history of atrial fibrillation). Baseline assessments included a comprehensive clinical assessment, transthoracic echocardiography, blood and urinary sample collection. Baseline uDKK3 concentrations were quantified in urine samples using an enzyme-linked immunosorbent assay (ELISA), normalized to urinary creatinine, and log-transformed to improve interpretability.
Patients underwent systematic follow-up after 12months to assess the primary endpoint of progressive renal dysfunction, defined as an annual decline in estimated glomerular filtration rate (eGFR) >0.75ml/min/1.73m², exceeding the expected age-related annual loss. Statistical analyses included the Mann–Whitney U and Chi-square tests for intergroup comparisons. UDKK3, plasma creatinine and α1-microglobulin were compared using a general linear model adjusted for age, sex, and BMI. Logistic regression analysis adjusted for demographic parameters was performed to assess the association between baseline urine markers and the primary endpoint.
Results
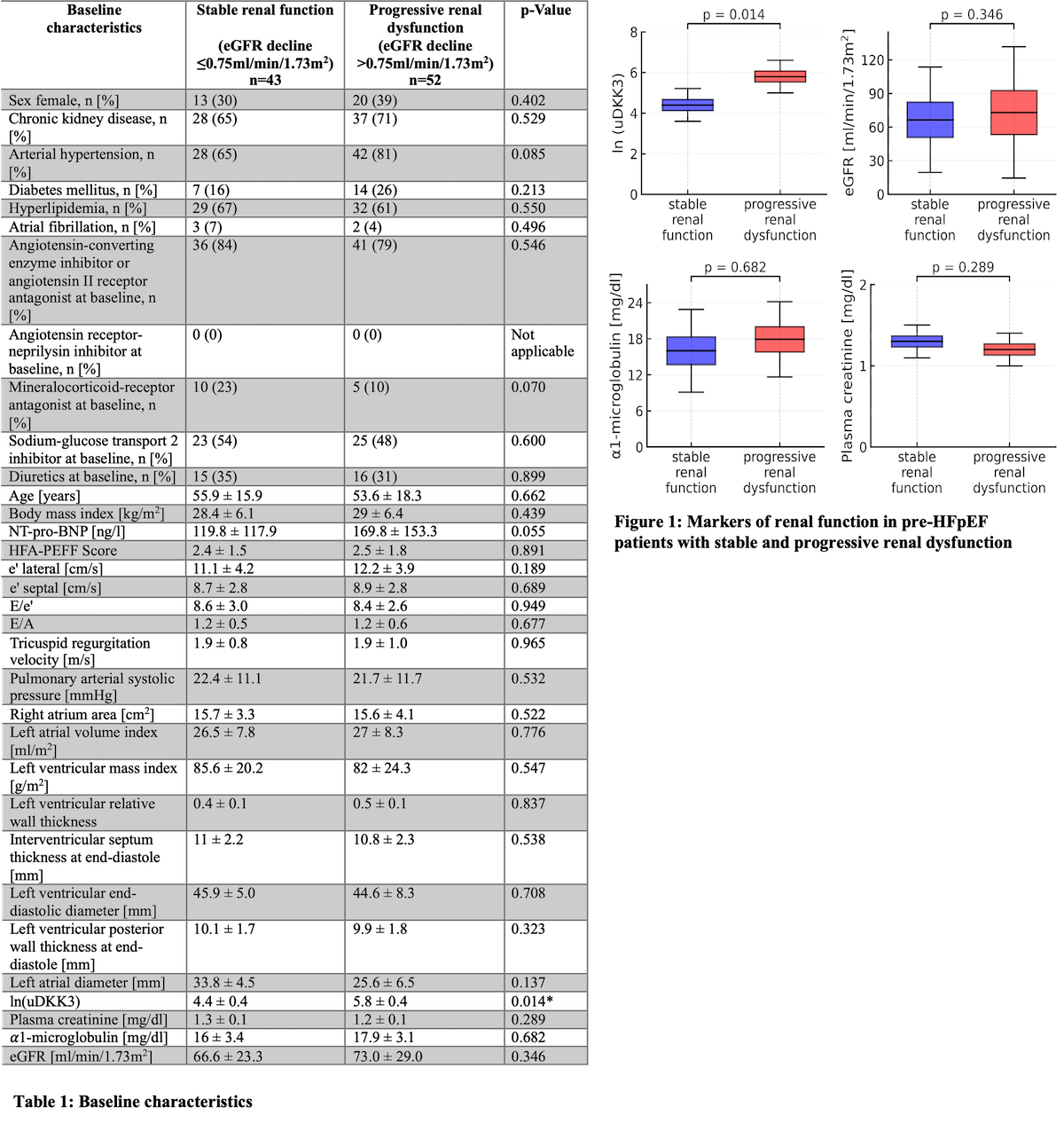
After exclusion of 3patients without baseline urine samples for uDKK3 analysis and 1patient lost to follow-up, the final cohort comprised 95patients (55±17 years, 33 [35%] female). During a median follow-up of 12.4months (IQR 12.0–13.3), 52patients (55%) had progressive renal dysfunction. Compared with patients with stable renal function, no significant differences were detected in baseline demographic characteristics, comorbidities, medication or echocardiographic parameters (Table 1). No differences in newly prescribed heart-failure medication were observed. Similarly, baseline eGFR, adjusted plasma creatinine and α1-microglobulin were comparable between groups (all p>0.05). However, adjusted ln-uDKK3 levels were higher in patients who developed progressive renal dysfunction (5.8 [95% CI 5.1-6.5] vs. 4.4 [95% CI 3.6-5.2]; p=0.014) (Figure 1).
In logistic regression analysis, ln-uDKK3 was the only independent predictor of progressive renal dysfunction (OR=1.76 per SD [95% CI 1.11-2.78]; p=0.017).
Conclusion
In pre-HFpEF patients, uDKK3 was the only predictor of renal functional decline while conventional renal and cardiac markers showed no differences compared to patients with stable renal function. UDKK3 may enable early recognition of emerging cardiorenal risk.