Background: Adipositas has been identified as both a driving and aggravating factor in the pathogenesis of atrial fibrillation (AF). Adipositas also has a significant impact on the treatment approaches of AF due to its influence on pharmacokinetics of anti-arrhythmic drugs and anticoagulation regimes.
Objectives: To analyse the ablation outcome and post-interventional management of anticoagulation in patients (pts) with obesity or severe adipositas and atrial fibrillation treated with catheter ablation
Methods: This is a retrospective single centre analysis of 1306 consecutive patients who received ablation therapy for atrial fibrillation (AF) or left atrial tachycardia (AT) at a large tertiary center. Pts were divided into two groups according to their BMI, group 1 (BMI 30.0-39.9 kg/m
2) and group 2 (>40 kg/m
2). Clinical data were analyzed according to ablation success and post-interventional management of anticoagulation and statistical analysis was performed with RStudio.
Results: 325 pts (male 64%) met the inclusion criteria (group 1 n=285, mean BMI 32.5 kg/m
2; group 2 n=40, mean BMI 43.7 kg/m
2). Most pts were treated for persistent AF or AT (71%), and 19% for paroxysmal AF or typical atrial flutter (10%). About half of the pts (n=150, 46%) received a 12-month follow-up (FU) visit, and 137/325 (42%) were followed for up to 55 months. 39.3% experienced arrhythmia recurrence within 12 months. There were no significant differences in the recurrence rate (52 pts (40.6%) in group 1, 7 (31.8%) in group 2 (p=0.586)). Similarly, the long-term recurrence rate beyond 12 months was 41% in group 1 and 59.1% in group 2 (p=0.167). Within the first 12 months, 39% of pts in group 1, and 32% of pts in group 2 required at least one reablation in order to obtain sinus rhythm at the 12-month FU visit.
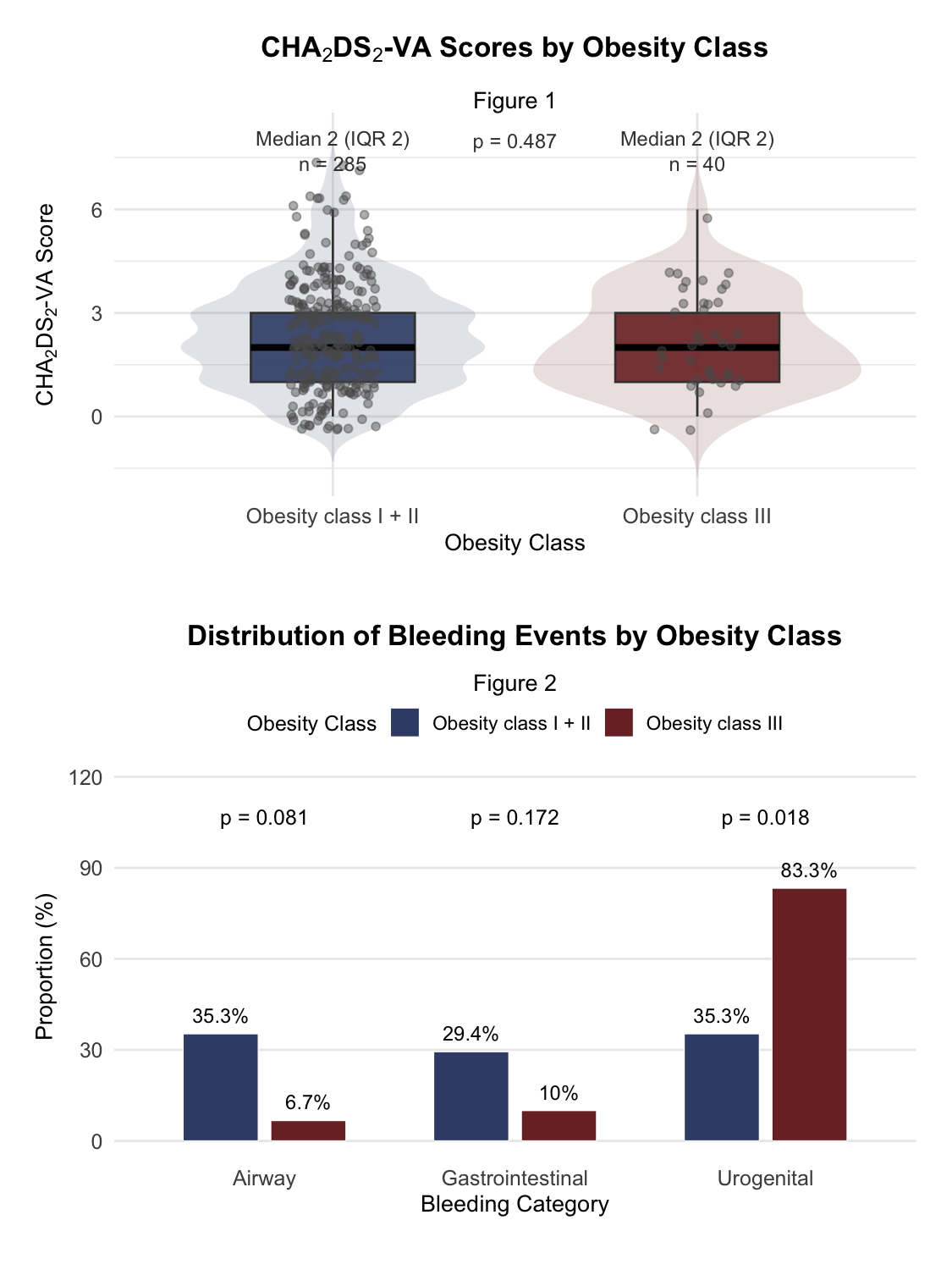
In both groups, the median CHA
2DS
2-VA-Score was 2 (Figure 1). Oral anticoagulation (OAC) discontinuation was comparable between both groups (10.9% vs. 9.1%; p=1.000; OR=1.04, 95% CI 0.25-4.31). Notably, no thromboembolic event occurred in pts with a CHA
2DS
2-VA-Score <2, regardless of OAC status. The overall incidence of thromboembolic event did not differ significantly between both groups (12.5% vs. 12.6%; p=1.000; OR=0.99, 95% CI 0.28-2.77), In contrast, the occurrence of bleeding events was higher in case of adipositas per magna compared to less severe adipositas (12.5% vs. 3.9%; p=0.034; OR=3.54, 95% CI 0.91-11.87). Most commonly, in group 2 urogenital bleeding occurred (Figure 2).
Conclusion: Our data show that overall there are no significant differences in the treatment success for obese and severely obese patients. Most notably, the efficacy of anticoagulation remains unfazed by severe overweight, and stopping the anticoagulation after ablation in severely obese patients seems beneficial due to comparable stroke incidence but a higher bleeding risk.