Background: Management of acute pulmonary embolism (PE) remains challenging, particularly in intermediate-high and high-risk patients. We hypothesized that the establishment of a multidisciplinary Pulmonary Embolism Response Team (PERT) would improve acute-phase outcomes through faster decision-making and the implementation of advanced therapeutic strategies.
Methods: We retrospectively analyzed 272 patients with confirmed PE (136 before and 136 after PERT implementation, 2015–2025) after propensity score matching for age, sex, and risk profile. Baseline characteristics, laboratory and echocardiographic parameters, therapeutic strategies, and in-hospital outcomes were compared between the groups.
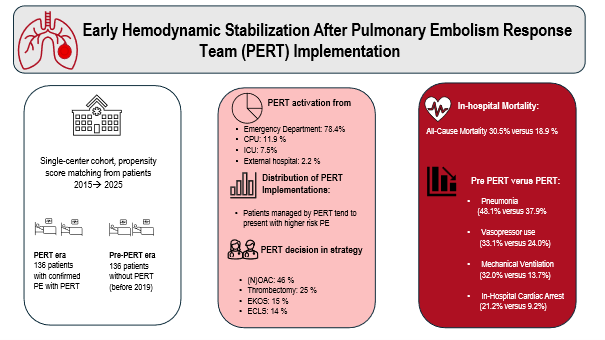
Results: Patients treated during the PERT era more frequently presented with intermediate-high or high-risk PE but received more advanced reperfusion therapies, including thrombectomy (25%), EKOS (15%), and ECLS (14%). Despite similar baseline characteristics, PERT implementation was associated with a significant reduction in vasopressor use (33.1% vs. 18.2%, p = 0.005), lower rates of mechanical ventilation (32.0% vs. 13.7%, p < 0.001), and fewer in-hospital cardiac arrests (21.2% vs. 9.2%, p = 0.007). In-hospital mortality decreased markedly from 30.3% before PERT to 18.9% after implementation (p = 0.036). Echocardiographic markers of right ventricular strain (TAPSE, RV/LV ratio, sPAP) showed overall improvement in the PERT era, indicating better hemodynamic stabilization.
Conclusion: The introduction of a structured, multidisciplinary PERT program led to significant hemodynamic stabilization, reduced need for advanced cardiopulmonary support, and lower in-hospital mortality in patients with acute PE. Our findings highlight the clinical impact of real-time multidisciplinary decision-making in acute PE care.
Graphical Abstract: