BackgroundWith long-term recurrence rates over 50% after catheter ablation, atrial fibrillation (AF) therapy is still not satisfactory. One likely reason is our limited understanding of individual AF mechanisms. This in turn, is in part owed to absence of mapping systems capable of assessing the spatio-temporal AF dynamics in a global, beat-to-beat fashion.
Slow conduction plays an important role in the AF pathomechanism. It is unknown, however, to what extent individual AF patterns are determined by local conduction velocities and how they impact the response to therapy.
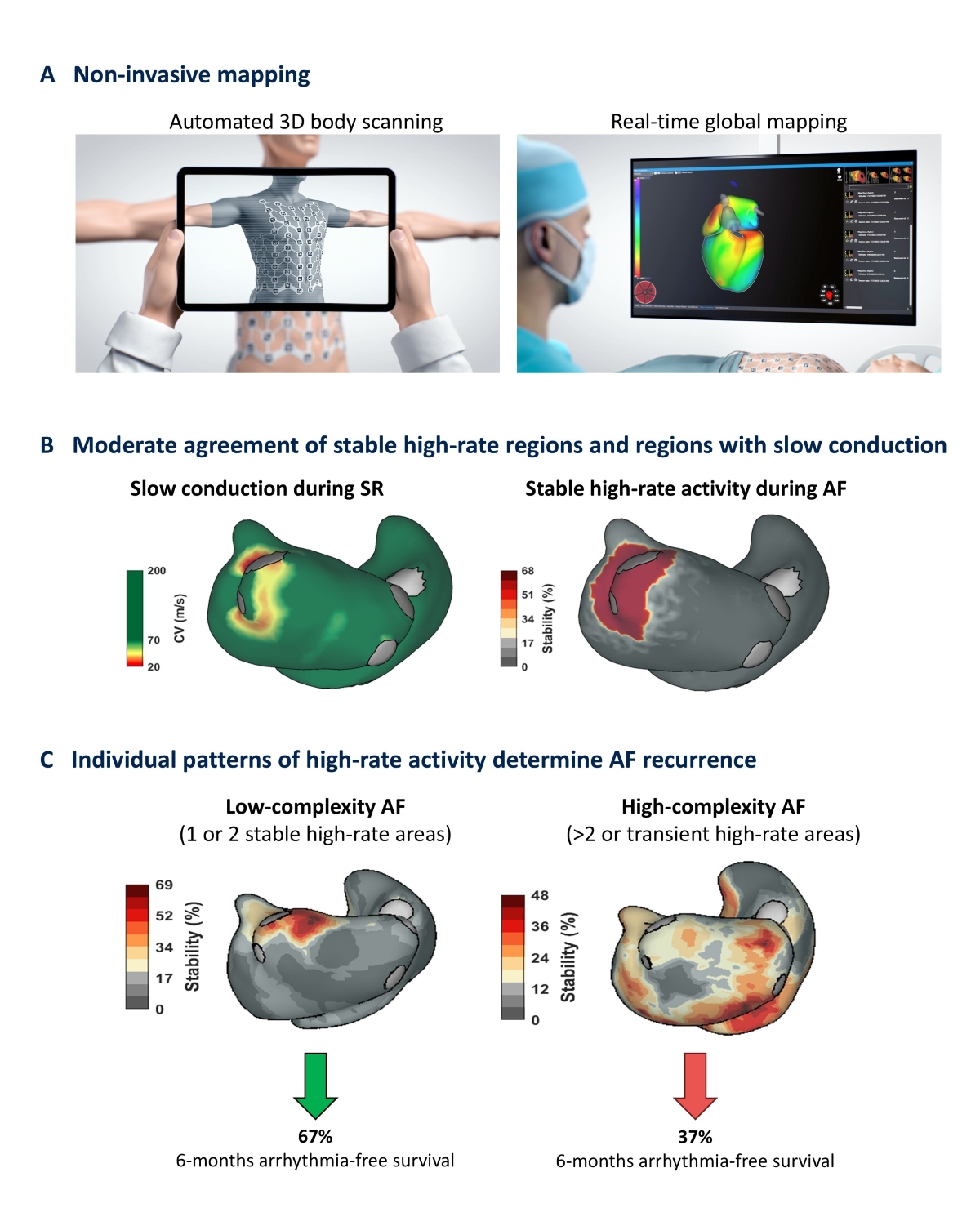
Here we use a novel non-invasive global mapping system which enables assessment of local conduction velocities and individual spatio-temporal AF dynamics (Fig. 1A). We aim to identify AF-perpetuating drivers that are stable over time and to link them to the underlying individual substrate and arrhythmia recurrence.
MethodsIn this prospective study consecutive patients undergoing electrical cardioversion were included. All patients received continuous non-invasive mapping before (AF) and after cardioversion (sinus rhythm). Critical AF drivers were defined as atrial sites with high-rate activity, over more than 50% of the recording time. In a regional analysis the localization of those Stable Atrial High-Rate Activity (SAHRA) sites was compared with the local conduction velocities and linked to arrhythmia-free survival over a 6-months follow-up.
Results 51 patients undergoing electrical cardioversion were prospectively included. Sites of stable high-rate activity were predominantly (67%) localized in regions that displayed slow-conduction (<0.5 m/s) during sinus rhythm (moderate agreement, interrater reliability κ=0,44; p<0,0001) (Fig. 1B). While the absence of regional slow-conduction rendered the presence of stable high-rate activity unlikely (negative predictive value: 95.3%), the positive predictive value was rather low (42.8%).
Based on the total number of stable high-rate activity sites in a given patient we distinguished complex AF patterns (>2 high-rate activity sites or no stable pattern at all) from non-complex AF patterns (1 or 2 sites of stable high-rate activity). Patients with complex AF patterns had a significantly lower 6-months arrhythmia-free survival after cardioversion than those with non-complex AF patterns (Fig. 1C). Moreover, complex AF pattern was an independent predictor of arrhythmia recurrence (OR 1.9, 95% CI 1.15-2.9, p=0.011; AUC 0.73, p=0.006).
ConclusionsAF-perpetuating stable high-rate activity preferably develops in regions that display slow conduction in sinus rhythm. The individual patterns of high-rate activity and their complexity are an independent predictor of arrhythmia recurrence after cardioversion. These data suggest that non-invasive global mapping may be a powerful tool to define individual AF phenotypes and to personalize AF therapy accordingly.