Background: This analysis compares the efficacy of pharmacological therapy with mavacamten and invasive alcohol septal ablation (ASA) in patients with hypertrophic obstructive cardiomyopathy (HOCM) in terms of clinical, echocardiographic, and patient-reported parameters over three months.
Methods: Seventy-nine patients (58 mavacamten, 21 ASA) were included from our prospective HCM registry. In addition to echocardiographic parameters (LVOT gradient at rest and under provocation, LV-EF, septal thickness), clinical and patient-reported parameters were collected using the KCCQ score before the start of therapy and after 3 months.
Results: At the start of the study, the groups were comparable in terms of age (61.6 ± 1.7 years vs. 57.3 ± 2.6 years; p = 0.18) and gender (male 51.7% vs. 61.9%; p = 0.42). Clinically, both groups showed a similar baseline distribution of NYHA class (II: 53% vs. 52%, III: 47% vs. 43%).
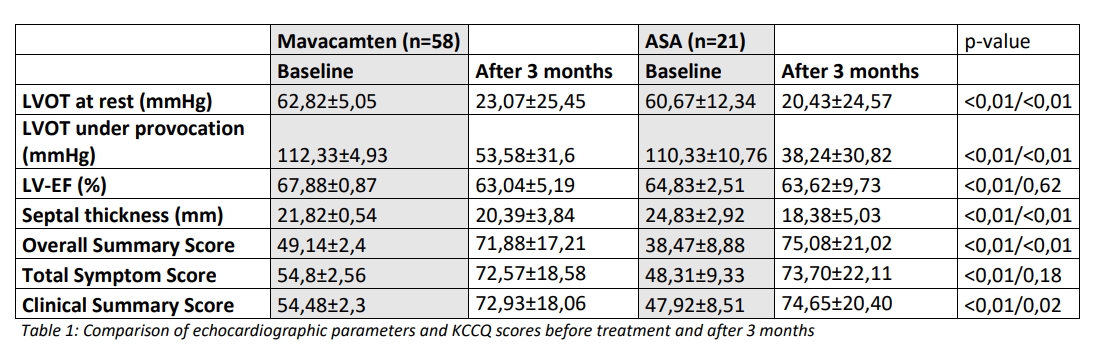
After three months, there was a significant improvement in functional capacity in both groups. Under mavacamten, 93% of patients were in NYHA I–II (I: 44.8%, II: 48.3%), and under ASA, 90% (I: 57.1%, II: 33.3%). The mean LVOT gradient at rest decreased from 62.8 ± 5.1 mmHg to 23.1 ± 25.5 mmHg with mavacamten and from 60.7 ± 12.3 to 20.4 ± 24.6 mmHg with ASA (p = 0.68). Under provocation, the gradient decreased from 112.3 ± 4.9 to 53.6 ± 31.6 mmHg with mavacamten and from 110.3 ± 10.8 to 38.2 ± 30.8 mmHg with ASA (p = 0.06). LVEF decreased slightly (mavacamten 67.9 → 63.0%, ASA 64.8 → 63.6%) but remained within the normal range. Septal thickness showed a greater decrease, particularly after ASA (24.8 → 18.4 mm; p = 0.11) compared to mavacamten (21.8 → 20.4 mm). One patient developed left ventricular dysfunction while taking mavacamten (4.9%), and seven patients developed a higher-degree AV block while ASA (33.3%); in two patients, this remained persistent, requiring pacemaker implantation (9.5%).
The KCCQ-23 results showed a significant improvement in quality of life in both groups. The overall summary score rose from 49.1 ± 2.4 to 71.9 ± 17.2 points with mavacamten and from 38.5 ± 8.9 to 75.1 ± 21.0 with ASA (p = 0.59). Comparable increases were found for the Total Symptom Score (mavacamten 54.8 → 72.6; ASA 48.3 → 73.7), the Clinical Summary Score (54.5 → 72.9 vs. 47.9 → 74.7), and the domains Quality of Life (QoL, 39.7 → 68.5 vs. 23.6 → 76.0) and social function (42.5 → 72.1 vs. 25.0 → 75.4).
Conclusion: Both mavacamten and ASA significantly improve symptoms, hemodynamic stress, and quality of life in HOCM and show comparable efficacy after three months. Mavacamten offers a well-tolerated, noninvasive, and clinically effective alternative to septal ablation.