Background. Over the last decades, outcomes of patients including high-risk and inoperable patients with symptomatic aortic valve stenosis (AS) were improved by transcatheter aortic valve implantation (TAVI). Despite continuous procedural advances in TAVI, a subset of patients experiences limited symptomatic benefit or poor survival after one year, indicating procedural futility. Detection of cardiac, extra-cardiac and procedural risk factors for these adverse outcomes is of paramount importance to identify these patients. This study aims to identify pre-existing and peri-procedural factors that predict futility one year after TAVI.
Methods. Between 2008 and 2023, 4,894 patients with severe AS undergoing TAVI at a single center were included in this analysis. Patients with valve-in-valve TAVI, concomitant valvular procedures, and early loss in follow-up were excluded. Independent predictors of all-cause mortality were assessed using Cox regression models at pre- and peri-procedural stages.
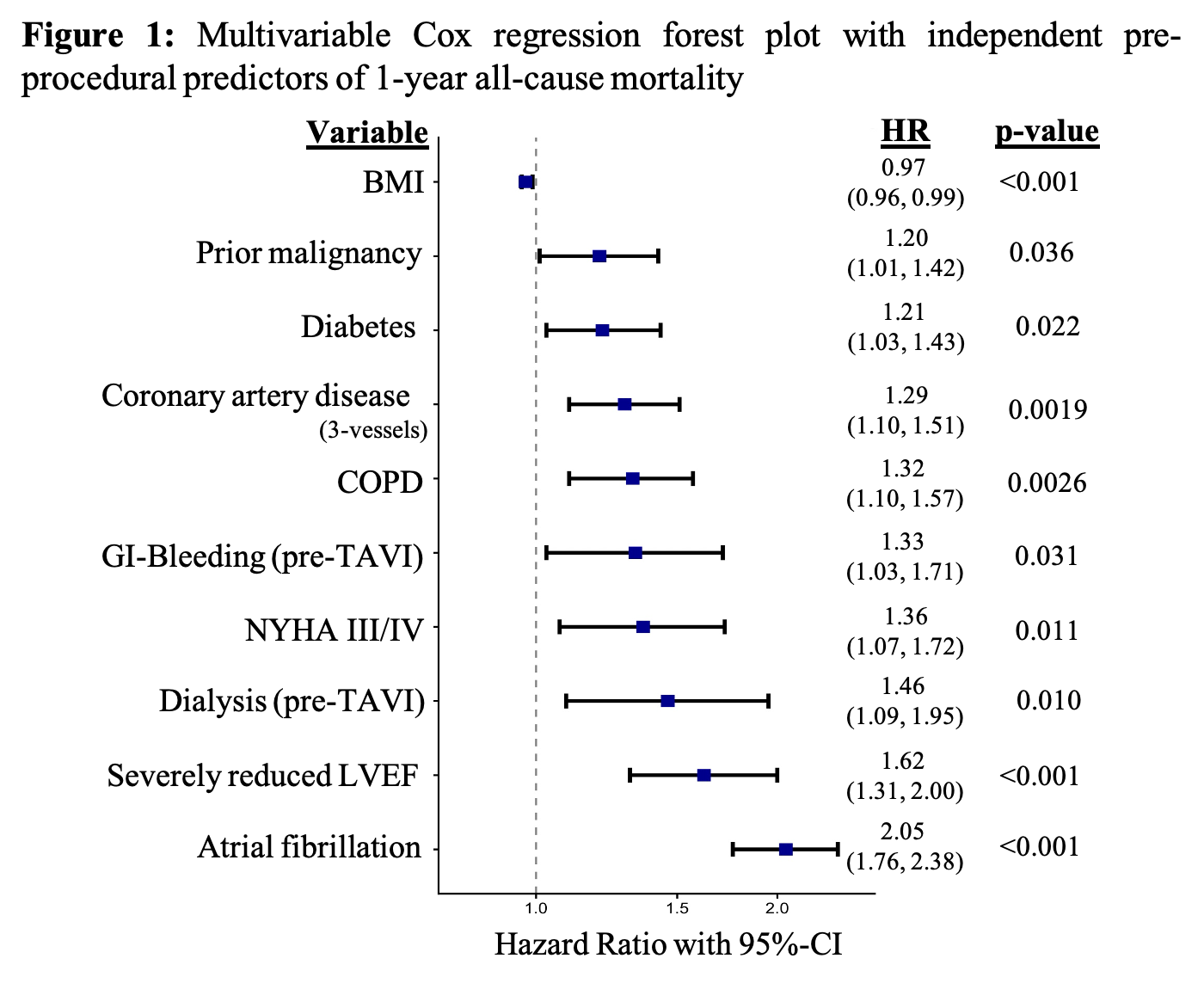
Results. Of 3,501 patients included in the final analysis, 777 patients (22.2%) died within the first year. Non-survivors were significantly more often male (55.3%; p=0.017), presented with lower body mass index (BMI) (p=0.024), higher rates of severe pulmonary hypertension (20%; p<0.001) and more significant concomitant tricuspid (11.4%; p<0.001) and mitral regurgitation (12.9%; p<0.001), as well as higher surgical risk scores (STS: 5.8%/EuroSCORE II: 5.7%; p<0.001). Median follow-up time was 5.1 years, with a 5-year mortality of 55.6%. According to multivariable analysis, chronic obstructive pulmonary disease (COPD) (hazard ratio [HR] 1.32; p=0.026), diabetes (HR 1.41; p=0.022), prior malignancy (HR 1.20; p=0.036), dialysis (HR 1.46; p=0.01), atrial fibrillation (HR 2.05; p<0.001), reduced left ventricular ejection fraction (LVEF≤30%) (HR 1.62; p=0.001), three-vessel coronary artery disease (HR 1.29; p=0.0019), NYHA class III/IV (HR 1.36; p=0.011) and history of gastrointestinal bleeding (HR 1.37; p=0.031) were identified as independent pre-procedural predictors of all-cause mortality after one year (
Fig. 1). Regarding peri-procedural risk factors, longer procedural time (HR 1.12; p=0.03) was identified as predictor for one year outcomes, as well as the choice of sedation:
Conscious sedation was associated with improved survival with a HR of 0.73 (p<0.001) compared to general anaesthesia. Transcatheter heart valve-type (balloon-expandable vs. self-expanding) did not affect survival after one year (HR 0.97; p=0.57).
Conclusion. In the herein investigated
all-comer TAVI cohort, adverse 12-months outcomes were mainly driven by systemic comorbidities. These findings emphasize that TAVI should not be offered to patients with advanced comorbidities and whose overall prognosis is poor with a life expectancy being unlikely to exceed 12 months. Especially, technically complex procedures with the need of conscious sedation or foreseeable longer procedural times should be avoided in these high risk patients to minimize
futile TAVI-interventions and thus enhancing long-term survival.