Background: Growing evidence indicates that total coronary plaque burden is a stronger predictor of major adverse cardiovascular events (MACE) than stenosis severity or ischemia detection. Coronary computed tomography angiography (CCTA), recommended as a first-line test for suspected chronic coronary syndrome (CCS), enables comprehensive quantification of coronary plaque volume. Recent studies have shown that the overall plaque burden - rather than its obstructiveness - primarily determines the risk of death and myocardial infarction. Patients with extensive non-obstructive plaque involvement experience event rates comparable to those with obstructive single-vessel disease. This study aimed to define CCTA-derived thresholds of total coronary plaque burden that predict or reliably exclude obstructive coronary artery disease (CAD) in an ESC guideline–based cohort.
Methods: This sub-analysis of the COPRODUCTION registry included patients who underwent clinically indicated CCTA at a German outpatient center between July 2017 and June 2020. Quantitative plaque analysis of all coronary arteries was performed using validated semi-automated software (syngo.via Frontier CT Coronary Plaque Analysis, version 5.0.2; Siemens Healthineers, Forchheim, Germany). Obstructive CAD was defined as ≥50% luminal diameter reduction in any coronary segment.
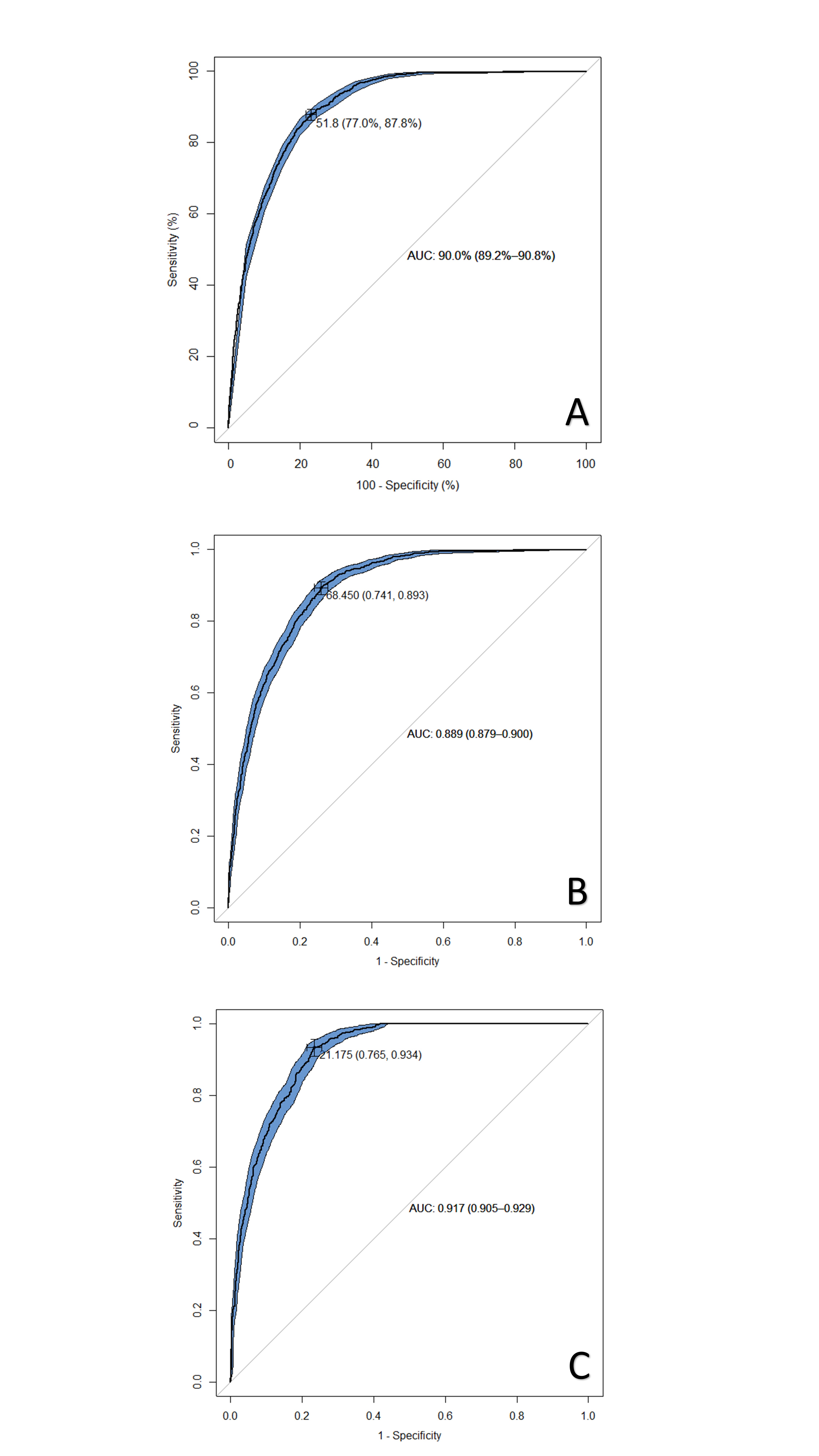
Results: This analysis included 5,412 patients (60.8% male; mean age 63 ± 11.5 years). Coronary plaques were detected in 3,629 patients (67.1%), and obstructive CAD in 1,584 (29.3%). Receiver operating characteristic (ROC) curve analysis for the presence of obstructive CAD yielded an area under the curve (AUC) of 0.90 for total coronary plaque burden. The Youden index identified an optimal cut-off of 51.85 mm³ (sensitivity 0.88, specificity 0.77). In sex-specific analyses, optimal cut-offs were 68.45 mm³ in males (sensitivity 0.89, specificity 0.74; AUC 0.89) and 21.18 mm³ in females (sensitivity 0.93, specificity 0.77; AUC 0.92).
For obstructive stenoses caused exclusively by calcified plaques, the AUC was 0.89 with an optimal cut-off of 27.65 mm³ (sensitivity 0.87, specificity 0.76). Sex-specific thresholds were 43.18 mm³ in males (sensitivity 0.84, specificity 0.78; AUC 0.88) and 18.15 mm³ in females (sensitivity 0.87, specificity 0.80; AUC 0.90).
The minimum plaque volumes associated with at least one significant stenosis were 22.0 mm³ in males and 12.4 mm³ in females, with a false-negative rate <5%. Patients below these thresholds typically had no stenoses.
Conclusions: Total coronary plaque burden showed excellent diagnostic performance for detecting obstructive CAD, with optimal cut-offs of 68.45 mm³ in males and 21.18 mm³ in females. For stenoses caused solely by calcified plaques, thresholds were lower. However, significant stenoses may occur even at low plaque volumes, highlighting the value of comprehensive quantitative plaque assessment in CCTA-based risk evaluation.
Receiver operating characteristic (ROC) curves for detecting obstructive coronary artery disease based on total coronary plaque burden (mm³) in the overall cohort (A), males (B), and females (C).