Introduction: Right (RBBB) and left bundle branch block (LBBB) are established markers of adverse outcomes in patients with cardiovascular disease, yet their prognostic significance in the general population remains uncertain due to inconsistent evidence. Therefore, this study aimed to (i) determine the prevalence of bundle branch block (BBB) at the population level, (ii) perform comprehensive cardiovascular phenotyping by risk factors and prevalent disease, and (iii) evaluate associations between BBB and a composite primary endpoint of all-cause mortality and cardiovascular disease.
Methods and Results: In total, 12-lead ECGs from 15,221 participants in the Hamburg City Health Study (HCHS), a population-based cohort of adults aged 45-74 years, enrolled since 2016, were analyzed. BBBs were defined by Minnesota Code criteria as complete or incomplete right (RBBB) or left (LBBB). Participants without BBB served as the reference group. The composite primary endpoint was all-cause mortality and incident cardiovascular disease (including heart failure, myocardial infarction, atrial fibrillation, pulmonary embolism, or stroke). Associations were assessed using Cox proportional-harzards models to estimate hazard ratios (HRs) with 95% confidence intervals (CIs).
Among 15,221 participants (50.7% male), complete LBBB was present in 128 (0.8%) and incomplete LBBB in 21 (0.1%), complete RBBB in 349 (2.3%) and incomplete RBBB in 323 (2.1%) participants. Individuals with BBB - except those with iRBBB - were older than those without BBB (median age in years: no BBB 60.0; cLBBB 66.5; iLBBB 66.0; cRBBB 68.0; iRBBB 58.0 years). The proportion of males was higher across BBB groups except for cLBBB (no BBB 49.4%; cLBBB 50.0%; iLBBB 81.0%; cRBBB 80.2%; iRBBB 72.1%). Hyperlipoproteinemia was more common in cLBBB and cRBBB (34.4% and 32.0%) than in those without BBB (22.6%) and prior myocardial infarction was more prevalent in cRBBB (7.5%) and cLBBB (8.7%) compared with no BBB (2.9%). Likewise, heart failure (HF) was more common in cLBBB (29.7%), cRBBB (21.1%), and iLBBB (28.6%) compared to controls (4.7%).
Median follow-up was 4.28 years (95% CI 4.26-4.31) for participants without BBB, 4.52 years (95% CI 4.23-4.88) for those with LBBB, and 4.39 years (95% CI 4.25-4.51) for RBBB. Both LBBB and RBBB were associated with increased risk of the composite primary endpoint (LBBB: HR 2.86, 95% CI 1.95-4.20, p<0.001; RBBB: HR 1.95, 95% CI 1.56-2.43, p<0.001) (Figure 1).
Conclusions: In this general population-based study, both cLBBB and cRBBB were associated with a higher prevalence of hyperlipoproteinemia, HF, and myocardial infarction, and with increased risks of all-cause mortality and incident cardiovascular disease. BBB thus signals adverse prognosis in the general population and supports enhanced risk stratification of asymptomatic individuals.
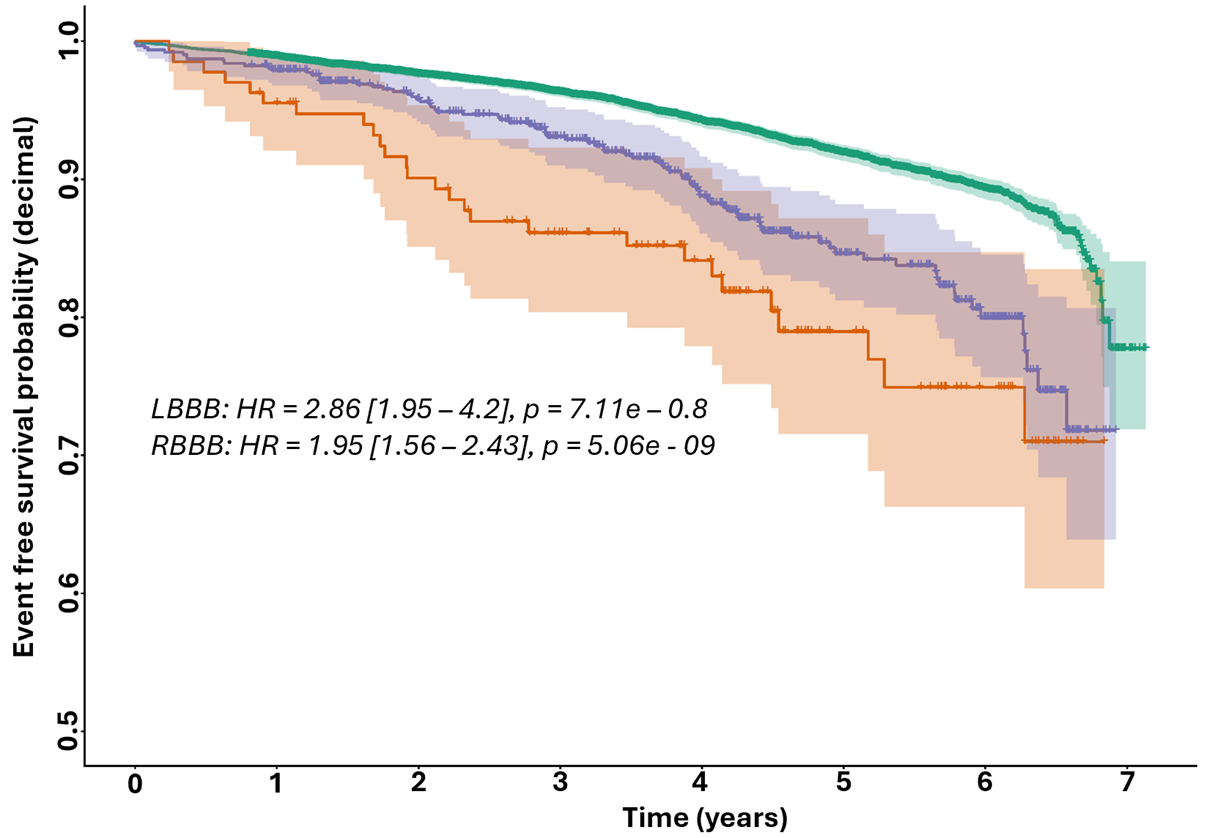
Figure 1: Kaplan-Meier estimates for the composite primary endpoint of all-cause mortality or cardiovascular disease. LBBB red, RBBB blue, No-BBB green.



