Introduction
Accurate detection of myocardial ischemia with vasodilator stress cardiovascular magnetic resonance imaging (S-CMR) relies on adequate hyperemia, typically induced pharmacologically with adenosine or regadenoson. To minimize false-negative results, current practice guidelines recommend monitoring clinical markers (heart rate (HR) increase >15 bpm or systolic blood pressure (SBP) drop >10 mmHg)1 as surrogate for adequate hyperemia. However, clinical response alone may not reliably reflect true myocardial hyperemia, and previous studies have shown that HR and SBP changes are rather poor surrogate markers for vasodilator-induced perfusion augmentation. Recently, a small study suggested quantitative myocardial blood flow (MBF) assessment (stress MBF ≥1.43 ml/g/min in ≥1 AHA segment) as a novel and superior marker for adequate hyperemia2. This study aimed to assess clinical and MBF response in a large real-world population of consecutive patients undergoing vasodilator S-CMR.
Methods and Results
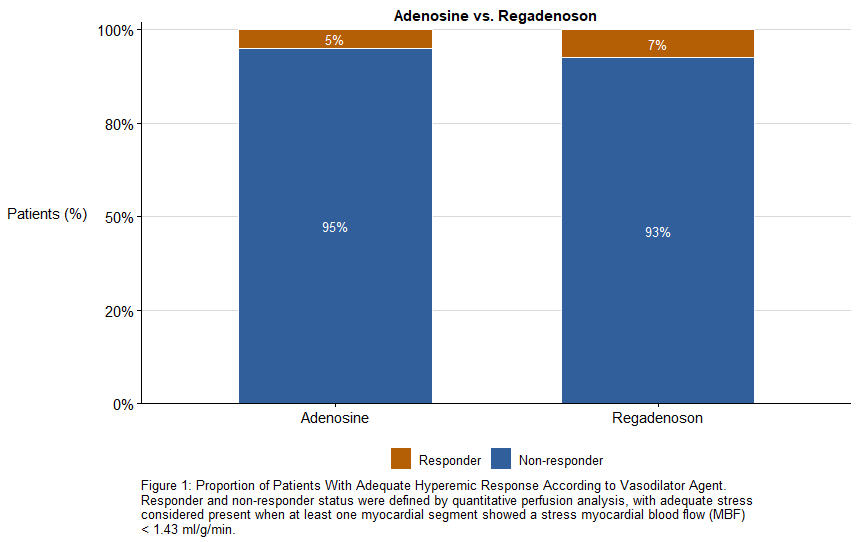
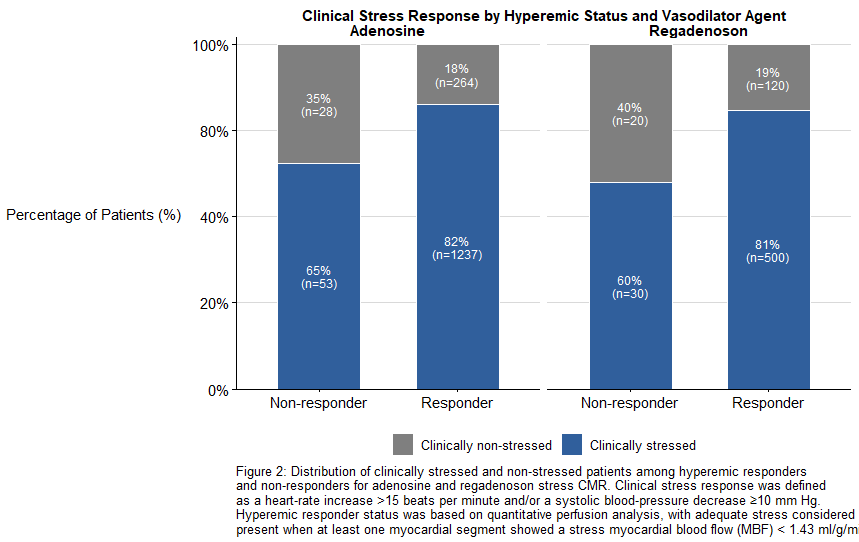
This was a retrospective secondary analysis of the Stuttgart Myocardial Perfusion Registry among 2,247 all-comer patients (age 65 ± 15, 64% male) who underwent S-CMR using either standard-dose adenosine infusion (140 µg/kg/min; n=1,577) or fixed-dose regadenoson bolus injection (400 µg; n=670). HR and SBP were recorded at rest and during vasodilator stress, and quantitative MBF was measured across all myocardial segments using automated inline pixel-wise perfusion mapping. Adequate hyperemia was defined as MBF ≥1.43 ml/g/min in ≥1 AHA segment as previously proposed2. Based on this criterion, 5% of adenosine and 7% of regadenoson studies demonstrated insufficient hyperemia. Among MBF-confirmed responders, 18% (adenosine) and 27% (regadenoson) did not meet clinical stress criteria. Conversely, 65% (adenosine) and 58% (regadenoson) of non-responders based on MBF still demonstrated clinical response in vital signs. Further subgroup analysis revealed no consistent association between any individual or combined vital parameters and the vasodilator response.
Conclusions
Clinical parameters such as HR and SBP changes do not reliably confirm adequate hyperemia during vasodilator S-CMR. Notably, 58–65% of patients with clinical stress responses failed to reach suggested stress MBF thresholds, indicating a substantial rate of insufficient stress both in clinical adenosine and regadenoson studies. These findings support the routine integration of quantitative perfusion analysis into clinical S-CMR protocols to ensure true hyperemic response is achieved and thereby improve diagnostic accuracy.
References
- Kramer, C. M. et al. Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update. J. Cardiovasc. Magn. Reson. Off. J. Soc. Cardiovasc. Magn. Reson. 22, 17 (2020).
- Kotecha, T. et al. Quantitative cardiovascular magnetic resonance myocardial perfusion mapping to assess hyperaemic response to adenosine stress. Eur. Heart J. - Cardiovasc. Imaging 22, 273–281 (2021).