Background: Severe mitral regurgitation (MR) is one of the most common valvular heart diseases in industrialized countries and is frequently associated with progressive left ventricular (LV) dilatation, systolic dysfunction and heart failure symptoms despite optimal medical therapy. In patients with advanced LV dysfunction and high surgical risk, transcatheter edge-to-edge repair (TEER) offers effective symptom relief and reverse remodelling yet may induce abrupt hemodynamic changes leading to afterload mismatch and acute LV failure. Levosimendan, a calcium sensitizer with combined inotropic and vasodilatory properties, may help mitigate this complication by improving contractility without increasing oxygen consumption. However, evidence supporting its use in this setting is scarce and heterogeneous.
Objective: To systematically evaluate the evidence on the effects of Levosimendan in patients with severe MR and LV dysfunction undergoing TEER, providing the first quantitative synthesis of existing data.
Methods: This systematic review and meta-analysis was conducted in accordance with PRISMA guidelines. A comprehensive search of PubMed, Embase, Scopus, and Google Scholar was performed up to September 15, 2025. Eligible studies included adult patients with severe MR and LV systolic dysfunction receiving pre- or peri-procedural Levosimendan during TEER. Primary outcomes were post-procedural LV ejection fraction (LVEF) and systolic pulmonary artery pressure (sPAP). Secondary outcomes included procedural success, procedure duration, and in-hospital complications. Data were pooled using random-effects models.
Results: Five studies published between 2016 and 2025 comprising 315 patients (141 receiving Levosimendan, 174 controls) met the inclusion criteria. The populations consistently represented high-risk cohorts with advanced heart failure and severely reduced LV function. Pooled analysis showed no significant difference in post-procedural LVEF between Levosimendan-treated patients and controls (mean difference 0.45%, 95% CI [−1.46 - 2.35] p=0.65) and no significant change from baseline (mean difference 1.10%, 95% CI [−2.22 - 4.42] p=0.52). Similarly, post-procedural sPAP did not differ significantly (mean difference 3.43 mmHg, 95% CI [−4.36 - 11.21] p=0.39). Procedural success was higher with Levosimendan (100% vs. 91.0%; p=0.006) and procedure duration was shorter (137.9 ± 48.2 vs. 181.6 ± 63.7 min; p<0.001). In-hospital mortality was low (1.0% vs. 0.0%; p=1.00), with comparable complication rates between groups.
Conclusions: This systematic review and meta-analysis suggests that Levosimendan may be associated with improved procedural performance in high-risk TEER patients, although no significant effects on early ventricular function were observed. The findings are hypothesis-generating and highlight the need for larger, prospective randomized trials to clarify the role of Levosimendan in this setting.
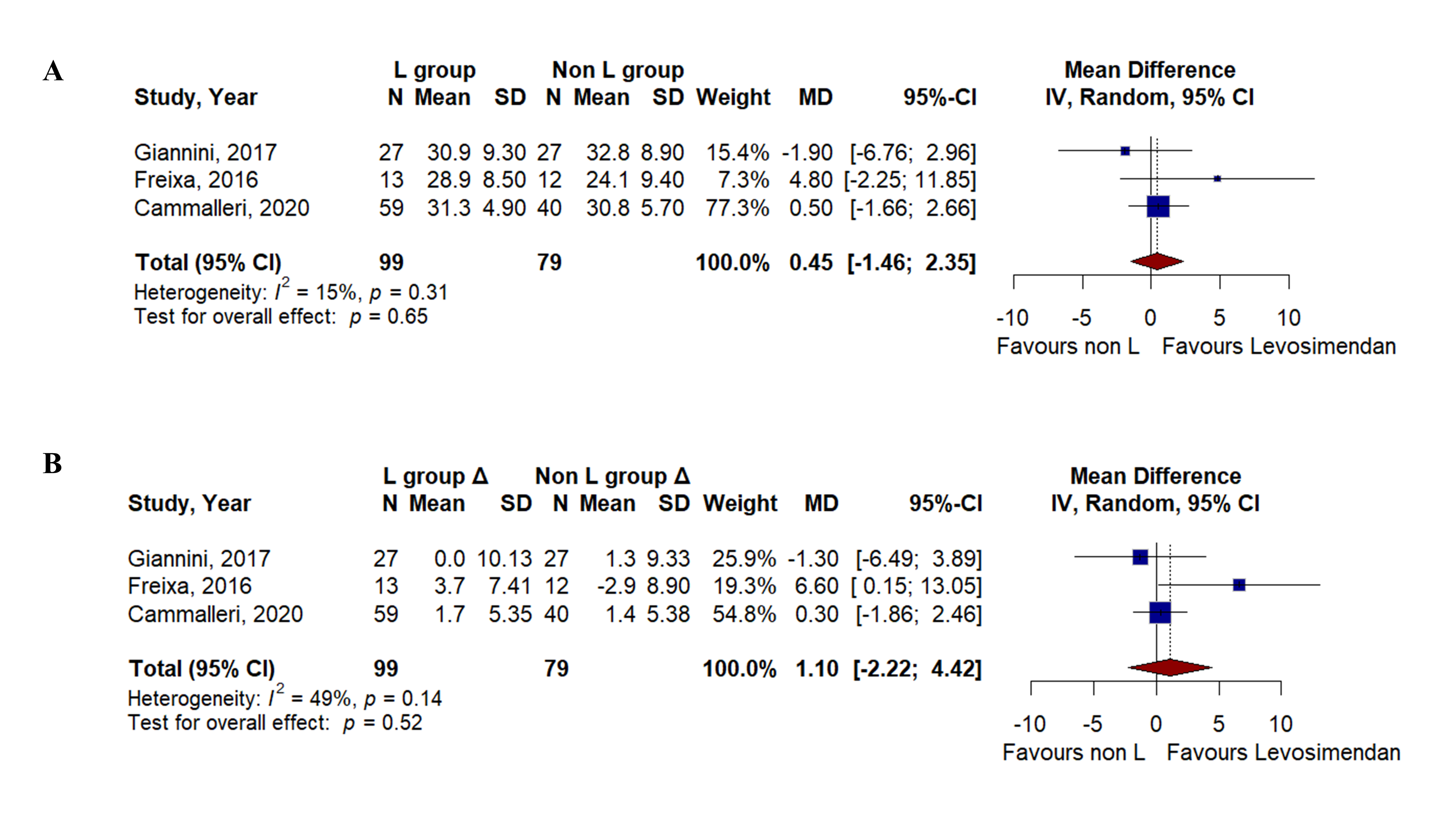
A.Pooled analysis of post-procedural left ventricular ejection fraction (LVEF) comparing L-group versus non-L group. B. Mean change (Δ) in LVEF from baseline to post-procedure in the Levosimendan group versus control group.



