Aims: Despite advances in transcatheter and surgical therapies, many patients with tricuspid regurgitation (TR) remain untreated or are referred too late. Existing risk models focus on procedural risk but ignore the substantial baseline risk of conservative management. We investigated whether combining predicted mortality risk under medical management with procedural risk estimation could support individualized treatment allocation.
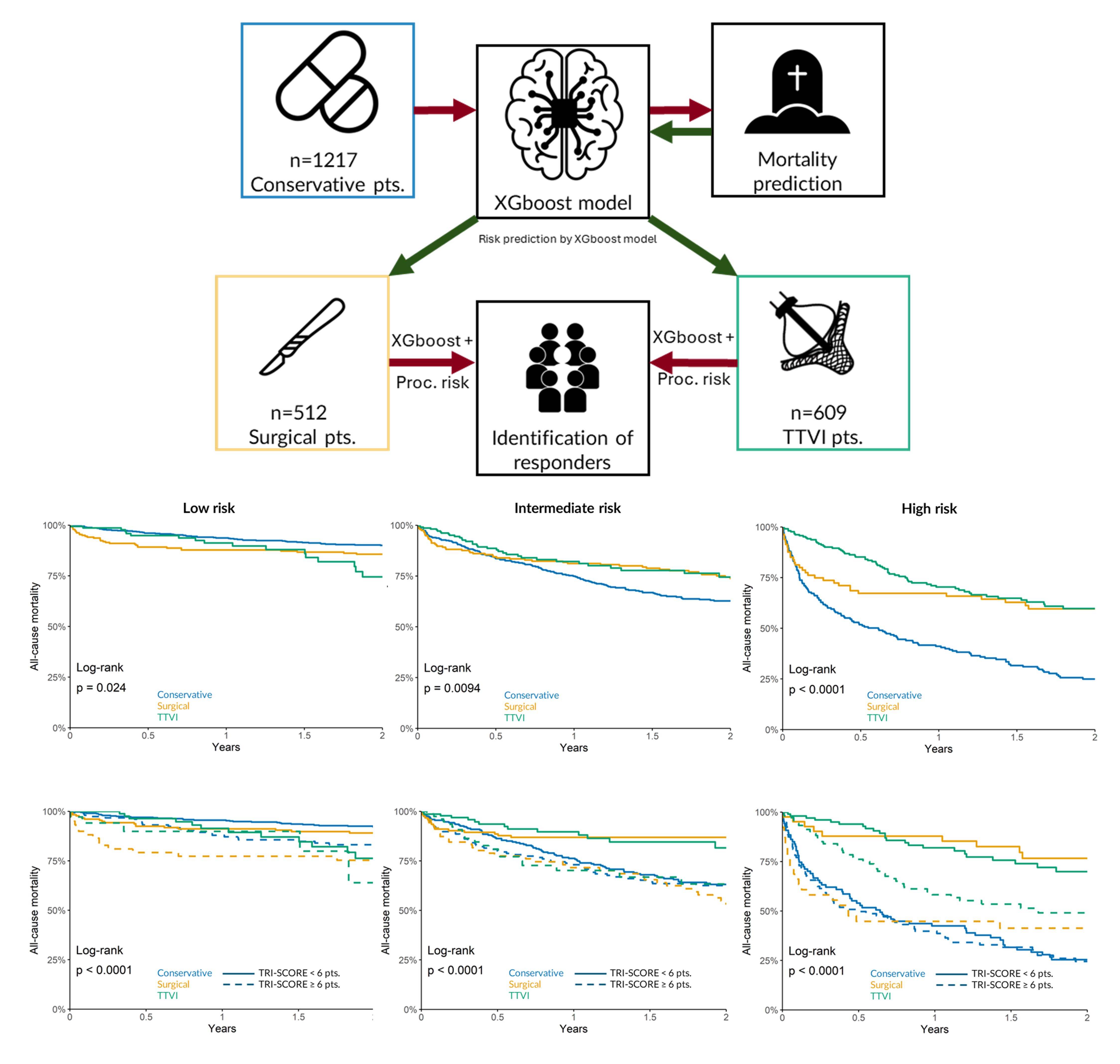
Methods: In the TRIGISTRY cohort, a gradient boosting model (XGBoost) was developed to predict 2-year all-cause mortality among conservatively managed patients. Model development followed an 80/20 training–test split with automated hyperparameter tuning and iterative feature elimination, removing predictors with <1% relative importance while monitoring performance (C-index) on the test set. The final model was selected based on cross-validated minimization of the Cox negative log-likelihood. Patients were stratified into low, intermediate, and high predicted mortality risk and outcomes were compared across treatment strategies: conservative management, transcatheter intervention (TTVI), or surgery. Procedural risk was further assessed by TRI-SCORE (<6 vs ≥6).
Results: Overall, 1,217 patients were treated conservatively (median age 74 years, 44% women), 512 underwent isolated surgery (70 years, 63% women), and 609 received TTVI (79 years, 58% women). The model effectively separated survival curves across risk strata (log-rank p<0.001).
Among low-risk patients (47% surgical, 26% TTVI), intervention did not confer a survival advantage compared with conservative treatment (2-year mortality: surgery 14%, TTVI 25%, conservative 10%; p=0.024). In intermediate-risk patients (38% surgery, 39% TTVI) and high-risk patients (16% surgery, 35% TTVI), both surgical and transcatheter therapies were associated with improved survival versus conservative management (intermediate: 26% and 26% vs 37%; high: 40% and 40% vs 75%; both p<0.01).
When stratified by TRI-SCORE, no treatment benefit was observed in the low-risk group irrespective of procedural risk. In the intermediate-risk category, both interventions improved survival in patients with TRI-SCORE <6, but not ≥6 (p<0.01). Among high-risk patients, both procedures improved outcomes in the low–intermediate TRI-SCORE group, whereas only TTVI provided a survival benefit in those with TRI-SCORE ≥6 (p<0.01).
Conclusion: A two-step strategy combining estimated mortality under conservative management with procedural risk enables individualized treatment decisions in TR. This approach supports optimal timing of intervention and helps identify patients most likely to benefit from tricuspid valve therapy.