Background: The long-term durability of transcatheter aortic valve implantation (TAVI) in bicuspid aortic valve (BAV) anatomy remains uncertain, with no randomised and limited long-term observational data. This is particularly relevant given the increasing use of TAVI in younger patients, where BAV disease is more prevalent. We aimed to characterise 5-year clinical and haemodynamic outcomes after TAVI in patients with BAV versus tricuspid aortic valve (TAV).
Methods: We retrospectively analysed consecutive patients undergoing TAVI with a balloon-expandable valve (Edwards SAPIEN 3 (Ultra)) between 01/2019-11/2020 at the University Medical Centre Mainz, with targeted 5-year follow-up. BAV morphology was adjudicated by echocardiography and cardiac computed tomography. Propensity score matching (1:1) was performed using age, sex (exact matching), baseline mean transvalvular gradient, aortic valve calcium score, left ventricular ejection fraction, EuroSCORE II and prosthesis diameter. The primary endpoint was the composite of valve-related long-term clinical efficacy defined by Valve Academic Research Consortium-3 (VARC-3) criteria, the secondary endpoint all-cause mortality. Time-to-event outcomes were analysed using Kaplan–Meier estimates and Cox models, categorical outcomes via logistic regression.
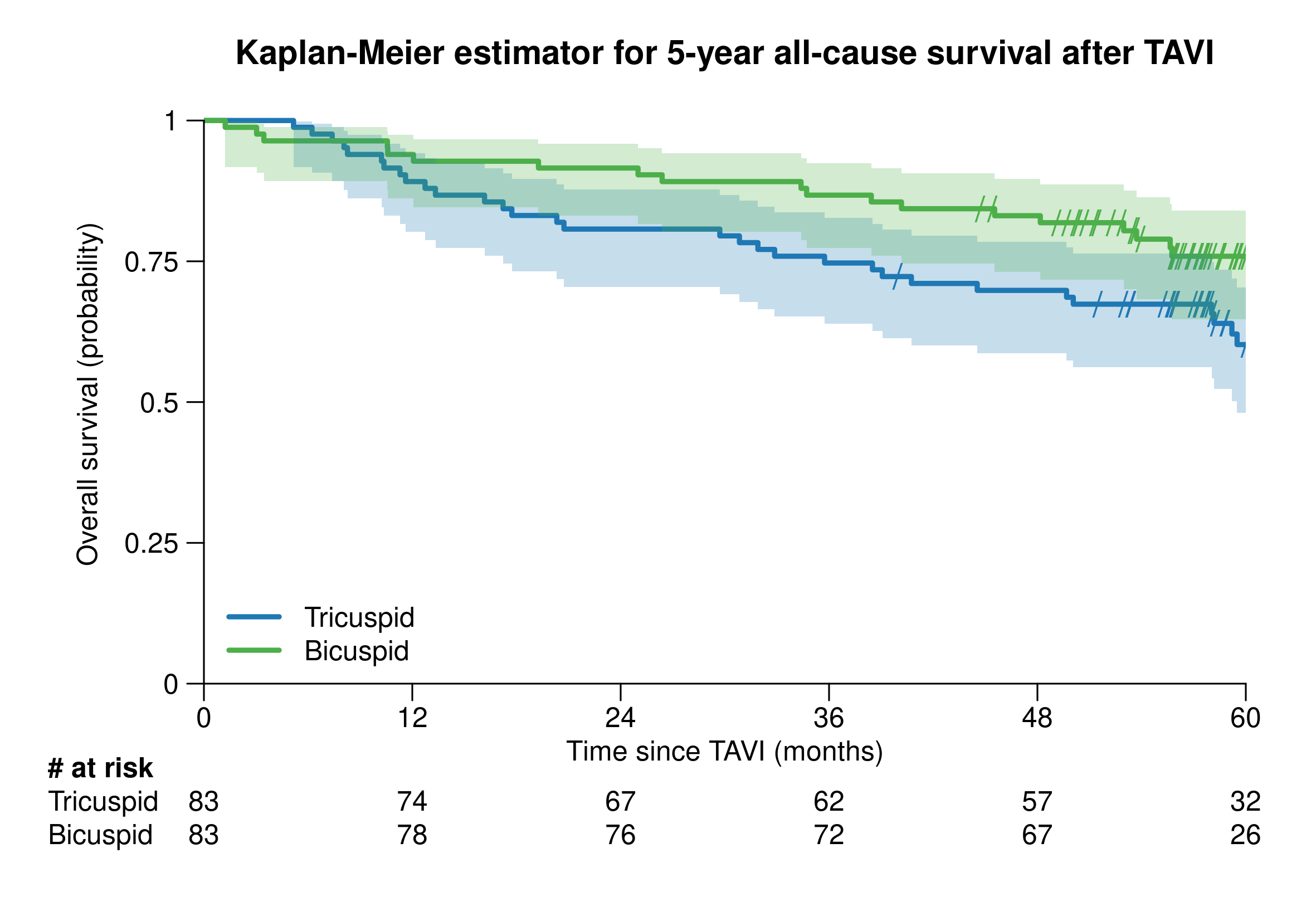
Results: Of 592 patients undergoing TAVI; 87 patients (14.7%) had BAV anatomy, of whom four were lost to follow-up. We analysed 83 matched pairs (BAV vs TAV) with comparable baseline characteristics (Table). BAV patients were younger than TAV patients (mean age 75 years) and of predominantly low surgical risk (EuroSCORE II 2.1%). Most had Sievers type 1 L–R morphology (~two-thirds), followed by type 1 R–N (~one-quarter). After a median follow-up of 4.9 years, valve-related long-term clinical efficacy among patients with available echocardiographic follow-up was higher in BAV (49/52, 94%) than in TAV patients (38/44, 86%, p = 0.034 by multivariable-adjusted logistic regression). This difference between the groups was driven by lower rates of valve-related mortality (0/52 vs 2/44) and stage 3 haemodynamic valve deterioration (0/52 vs 2/44), while re-operation/re-intervention rates were similar (3/52 vs 2/44). All-cause mortality did not differ between groups (Hazard Ratio for BAV vs. TAV 0.65, 95% CI 0.29 – 1.54; Figure).
Conclusion: In this matched cohort, patients with BAV undergoing TAVI showed at least comparable valve related clinical efficacy and all-cause survival to those with TAV at 5 years.
Table. Baseline characteristics and 5-year clinical outcomes after TAVI of 83 matched pairs of patients with bicuspid and tricuspid valve anatomy
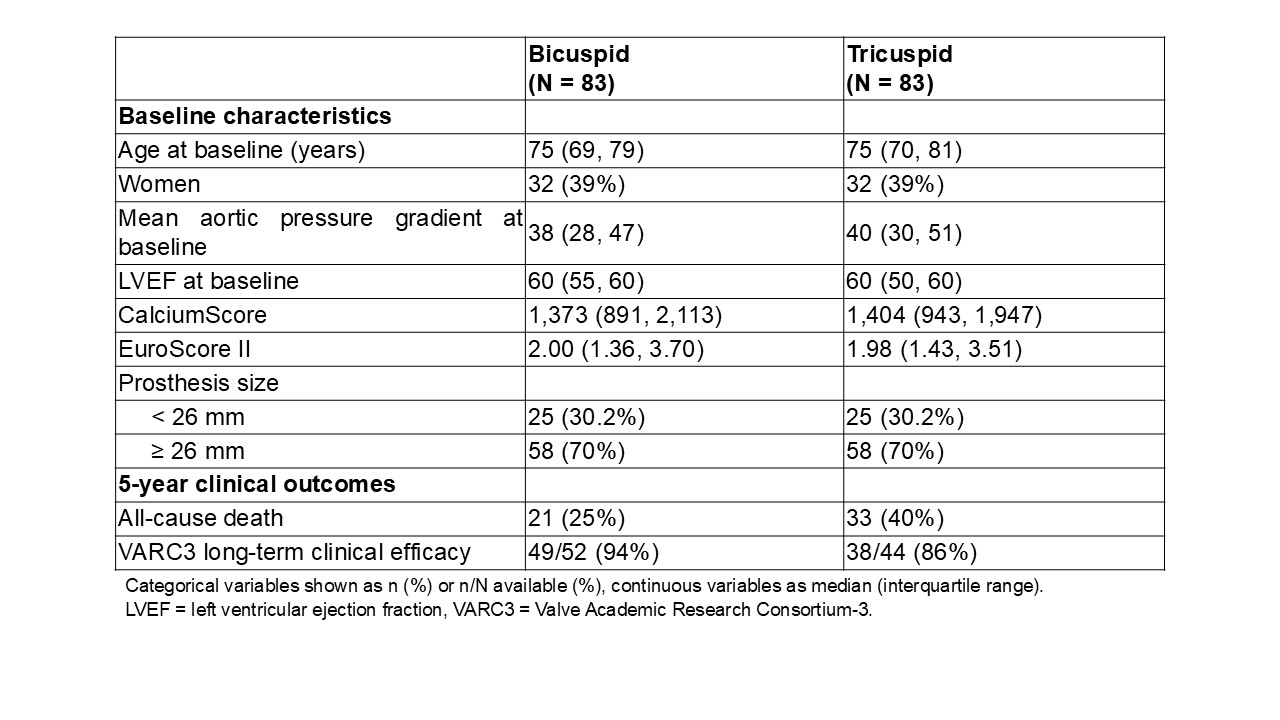
Figure. Kaplan-Meier estimator for 5-year all-cause survival after TAVI in matched pairs of patients with bicuspid and tricuspid valve anatomy.