Background: Approximately 30% of patients presenting with suspected myocardial infarction (MI) remain in the observe group. These patients are at high risk for mortality and major adverse cardiovascular events (MACE), making early risk stratification crucial. High-sensitivity C-reactive protein (hs-CRP) is a strong prognostic biomarker which has been recently evaluated in different patient groups and may be useful in this setting.
Methods: Patients presenting with suspected MI were prospectively enrolled and measurements of high-sensitivity cardiac Troponin I (hs-cTnI) and hs-CRP were obtained as well as GRACE-Score (1.0) calculated in each patient. After exclusion of STEMI patients and individuals with infectious cause of hs-CRP elevation, patients were categorized using the 0/1h hs-cTnI algorithm into three groups: Rule-in, observe, or rule-out. Quintiles of hs-CRP were defined for the observe group. All-cause mortality and MACE (defined as composite of cardiac death, MI, revascularization and cardiac rehospitalization) at 90 days, 1, 3, and 5 years were assessed. Event rates, Cox-regression, and c-indices were computed for hs-CRP, GRACE-Score, and their combination, adjusted for age, sex and cardiovascular risk factors.
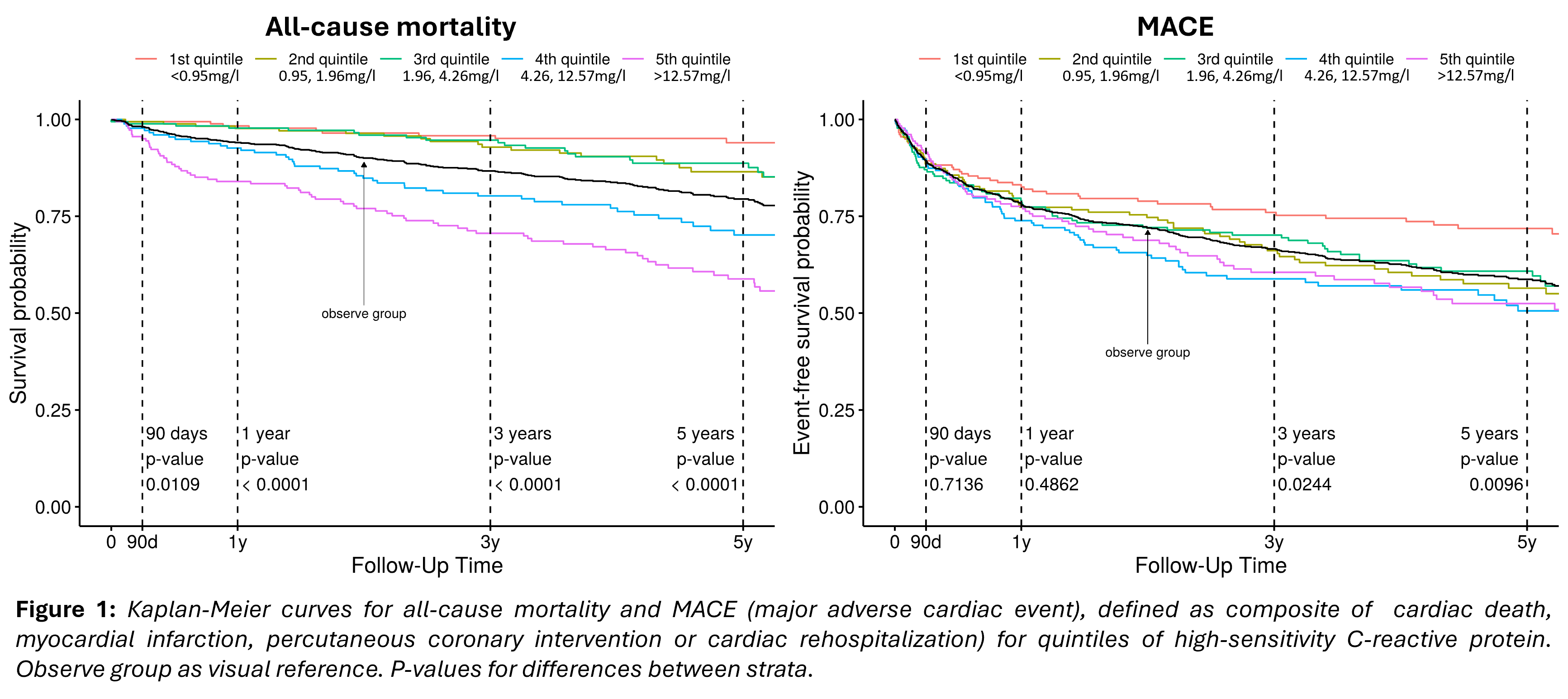
Results: Among 2,843 patients (median age 63 years; 36.1% female), 917 remained (32.3%) in the observe group. Median hs-CRP concentration in the observe group was 2.9 mg/l. Patients with hs-CRP concentrations in the highest quintile (> 12.57 mg/l) had significantly higher 1-year (16% vs. 1.7%), 3-year- (29.4% vs. 4.2%) and 5-year mortality (41.2% vs. 6%) as well as 3-year- (39.5% vs. 24%) and 5-year MACE (47.5% vs. 28.2%) compared to the lowest quintile (< 0.95 mg/l) (Figure 1). Hs-CRP resulted in a slightly higher c-index compared to the GRACE-Score for 3-year (C-index 0.787 vs. 0.737) and 5-year mortality (C-index 0.776 vs. 0.732). Combined interpretation of hs-CRP and GRACE Score even further improved model performance (C-index5-year mortality 0.794). Regarding MACE, no relevant differences between hs-CRP quintiles and GRACE Score could be identified. Elevated hs-CRP concentrations in the highest quintile independently predicted 1-year- (adjusted HR1-year 6.72 [2.03, 22.23], p = 0.002), 3-year- (adjusted HR3-years 5.37 [2.42, 11.93], p < 0.001) and 5-year mortality (adjusted HR5-years 6.44 [95%CI 3.07–13.50], p < 0.001) as well as 5-year MACE (adjusted HR 1.57 [95% CI 1.06, 2.31], p = 0.023) compared to the lowest quintile.
Conclusion: Hs-CRP is a strong independent predictor of mortality and MACE in patients with suspected MI, classified into the observe group, and improved risk-prediction beyond established models.