Background
Approximately 1 million cardiac implantable electronic devices (CIED) are implanted worldwide annually. Despite therapeutic benefits, these systems carry risks of malfunction and infection necessitating transvenous lead extraction (TLE). Despite advances in extraction techniques, TLE remains high-risk with major complication rates of up to 2%, including vascular tears requiring immediate surgical intervention. Consensus statements advocate settings with immediate surgical backup for high-risk cases. Yet, comparative study data show equivalent safety outcomes in well-equipped electrophysiology (EP) laboratories with surgical backup protocols. Evidence-based stratification is needed to guide safe EP laboratory extraction.
Objectives
This systematic review and meta-analysis aimed to identify evidence-based predictors for stratifying patients suitable for safe TLE in EP laboratories without immediate surgical standby.
Methods
Systematic searches of PubMed, ClinicalTrials.gov, and Cochrane Central were conducted from inception to October 2025, following Cochrane methodology. Two independent reviewers screened and extracted data from prospective and retrospective studies using standardized forms. Risk of bias was assessed with the Cochrane tool. Odds ratios (OR) were calculated as effect measure, with pooled estimates derived using generic inverse-variance and random-effects models. Heterogeneity was assessed by I², τ², and Cochrane’s Q. Sensitivity analyses excluded small or outlier studies and compared random- with fixed-effects models.
Results
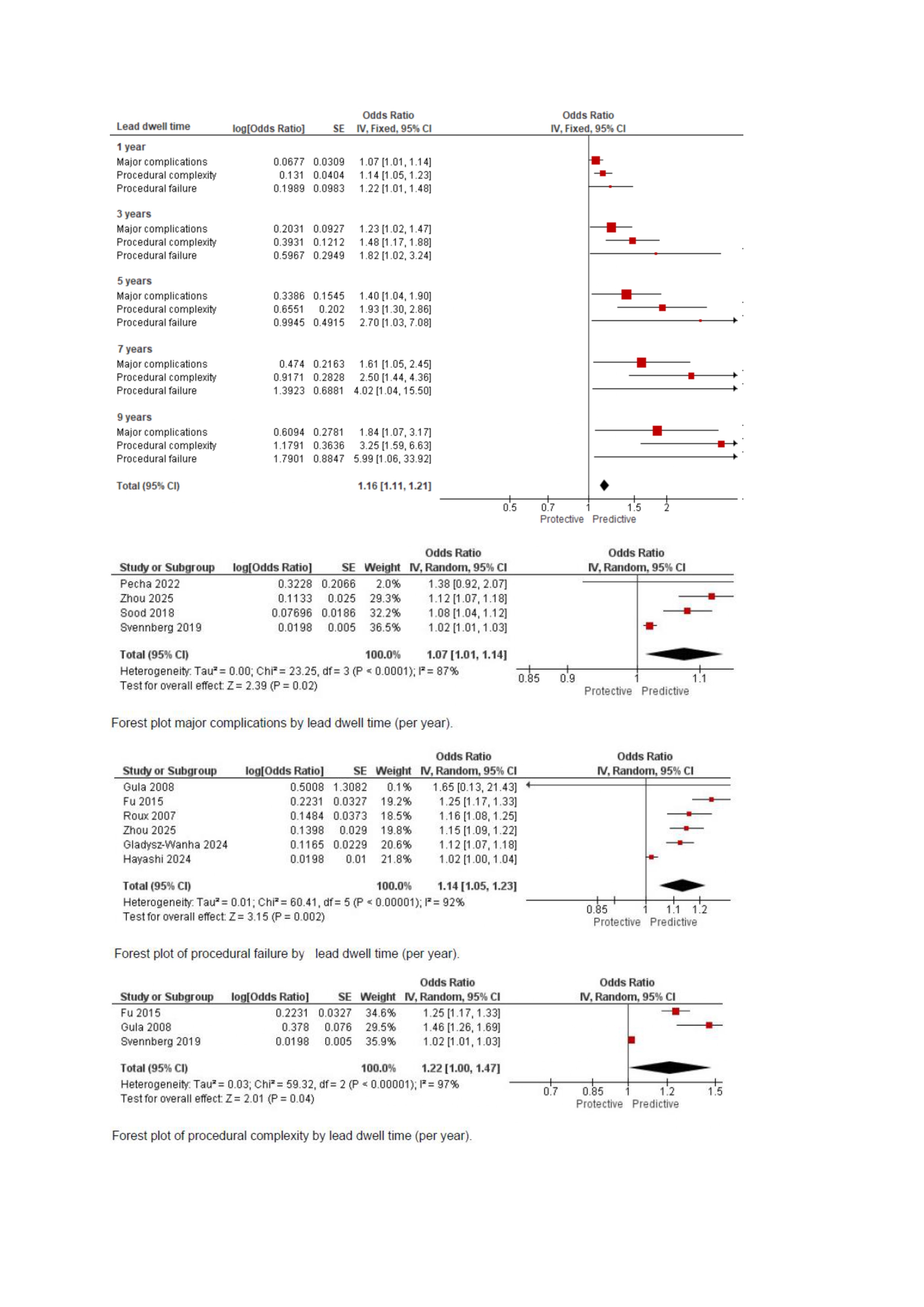
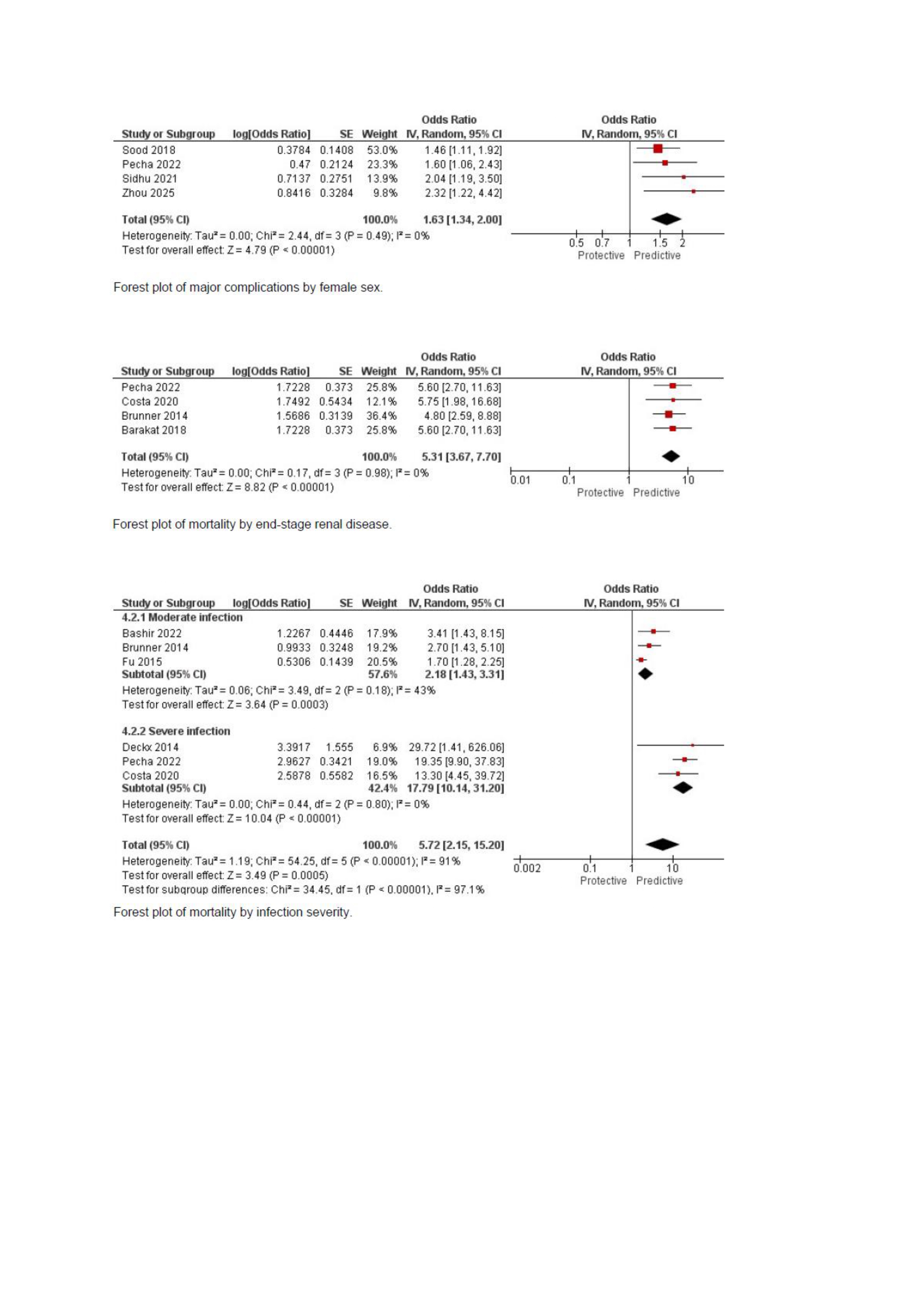
Database searches yielded 698 publications. 25 publications from 23 studies (9 prospective, 14 retrospective) met inclusion criteria, encompassing 39,051 patients. Meta-analysis of 18 publications synthesized in 24 comparisons identified distinct risk profiles. Lead dwell time independently predicted major complications (OR 1.07 [1.01-1.14]), procedural complexity (OR 1.22 [1.00-1.47]), and procedural failure (OR 1.14 [1.05-1.23]). ICD lead extraction strongly predicted procedural complexity (OR 3.31 [1.32-8.32]) but not failure (OR 1.30 [0.93-1.83]). Passive lead fixation predicted complex procedures (OR 1.71 [1.28-2.27]). Female sex (OR 1.63 [1.34-2.00]) and abandoned leads (OR 1.85 [1.12-3.05]) were associated with major complications, while CIED infection showed no association with complications (OR 0.88 [0.30-2.54]). Independent mortality predictors included chronic kidney disease (OR 1.67 [1.09-2.55]) and end-stage renal disease (OR 5.31 [3.67-7.70]), infection severity (moderate: OR 2.18 [1.43-3.31]; severe: OR 17.79 [10.14-31.20]), and age (OR 1.04 [1.03-1.05]).
Conclusions
Lead dwell time consistently predicts adverse outcomes in TLE. Additional lead characteristics are independent predictors for procedural failure and major complications. Mortality was shown to be driven by patient comorbidities rather than device characteristics. These findings support preprocedural risk stratification by lead characteristics to identify cases suitable for TLE in EP laboratories. For non-ICD leads with active fixation and dwell times < 6 years, likelihood of complications and procedural failure is acceptable for free-standing EP settings. Further research is needed to validate risk thresholds for venue selection.