Background: Obstructive Hypertrophic Cardiomyopathy (oHCM) is the most common primary cardiomyopathy. Data on comorbidities, treatment, as well as potential disparities, remain limited. This study analysed the characteristics of patients with oHCM in a large, population-based German cohort.
Methods: German health insurance claims data from 4.4 million individuals were analysed. Patients with oHCM were compared with an age- and sex-matched 1:10 control cohort. Multivariable logistic regression analyses identified factors potentially associated with the standard of care (SOC), including individual- and area-based socioeconomic factors, comorbidities, and comedications.
Results: Compared with the matched cohort, patients with oHCM had a significantly higher likelihood of being diagnosed with diseases defining the metabolic syndrome (Fig. 1A). Likewise, complications of metabolic syndrome occurred more frequently than in the matched cohort (Fig. 1B). 55% of patients with oHCM had coronary artery disease (vs. 24%, OR 4.01, p < 0.0001), 30% peripheral arterial occlusive disease (vs. 20%, OR 1.77, p < 0.0001), 28% chronic kidney failure (vs. 13%, OR 2.60, p < 0.001) and 16% sleep apnoea syndrome (vs. 9%, OR 2.01, p < 0.001).
HCM-related comorbidities were more prevalent in the oHCM cohort (Fig. 1C): sudden cardiac death (SCD, 6% vs. 2%, OR 3.58, p < 0.0001), syncope (17% vs. 8%, OR 2.25, p < 0.0001), mitral valve regurgitation (41% vs. 12%, OR 5.05, p < 0.0001), atrial fibrillation and flutter (39% vs. 16%, OR 3.31, p < 0.0001), and stroke (29% vs. 19%, OR 1.76, p < 0.0001). Despite this, only 57% consulted a cardiologist, 75% received beta-blockers, and 15% received non-dihydropyridine calcium channel antagonists. Receiving SOC was significantly and strongly associated with living in an area with higher income taxes (aOR 5.75, 95% CI 3.11 – 10.59) and a densely populated area (aOR 1.33, 95% CI 1.08 – 1.65). Interestingly, oHCM-associated comorbidities, such as mitral valve regurgitation (aOR 2.42, 95% CI 2.21 – 2.64) and atrial fibrillation and flutter (aOR 1.78, 95% CI 1.63 – 1.95), were also significantly associated with a higher likelihood of receiving SOC. Patients affected by a mental illness, specifically suffering from psychiatric diseases other than depression and anxiety (aOR 0.79, 95% CI 0.72 – 0.86) and depression (aOR 0.72, 95% CI 0.65 – 0.80) had a lower likelihood of receiving SOC.
Conclusion: Patients with oHCM show a very high burden of cardiovascular comorbidities and are undertreated. Patients residing in areas with higher income tax levels are more likely to receive SOC, whereas the presence of mental illnesses, such as depression, is associated with a lower likelihood of receiving SOC. This analysis suggests important areas for improving the care of patients with oHCM.
Figure 1
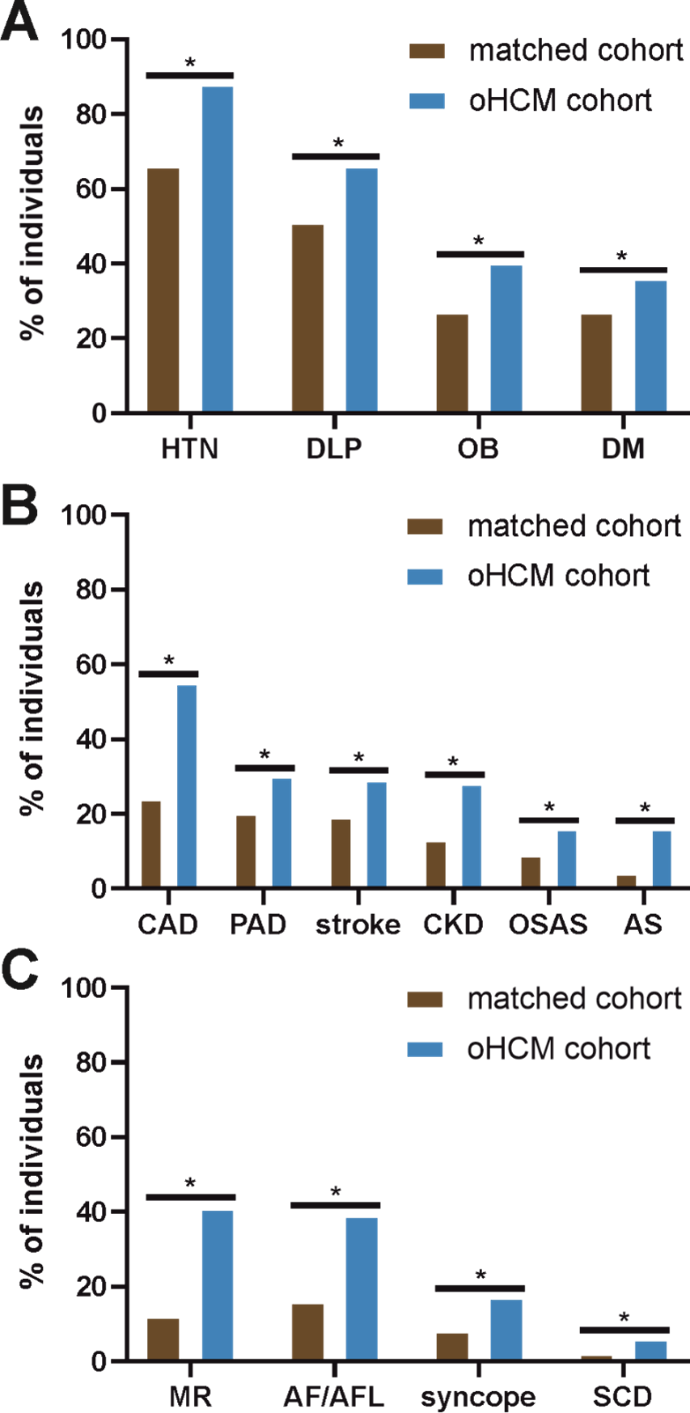
Figure 1 A-C Comparison of cardiovascular comorbidities in oHCM vs. the matching cohort. A: Metabolic-syndrome components: oHCM vs. controls. B: Impact of metabolic syndrom: oHCM vs. controls. C: oHCM-associated comorbidities vs. controls.



