Background
Several studies have compared current atrial fibrillation (AF) ablation modalities and identified elevated Body-Mass-Index (BMI) as a predictor of arrhythmia recurrence, evidence on procedural and clinical outcomes across BMI subgroups pertaining to different techniques remains limited.
Methods
This retrospective multicenter analysis included a cohort of consecutive patients undergoing first-time pulmonary vein isolation (PVI) with Pulsed-field ablation (PFA, Farapulse), Cryoballoon ablation (CBA), or high-power short-duration Radiofrequency ablation (RFA) in three electrophysiology centers from 2020 to 2024. Patients were stratified into 3 BMI groups (normal weight: <25; overweight: 25-<30, obese: ≥30 kg/m²). The primary endpoint was freedom from AF recurrence after 12 months following an 8-week blanking period. Secondary endpoints comprised procedural parameters (procedure and fluoroscopy time and radiation dose) as well as safety parameters (major and minor periprocedural complications).
Results
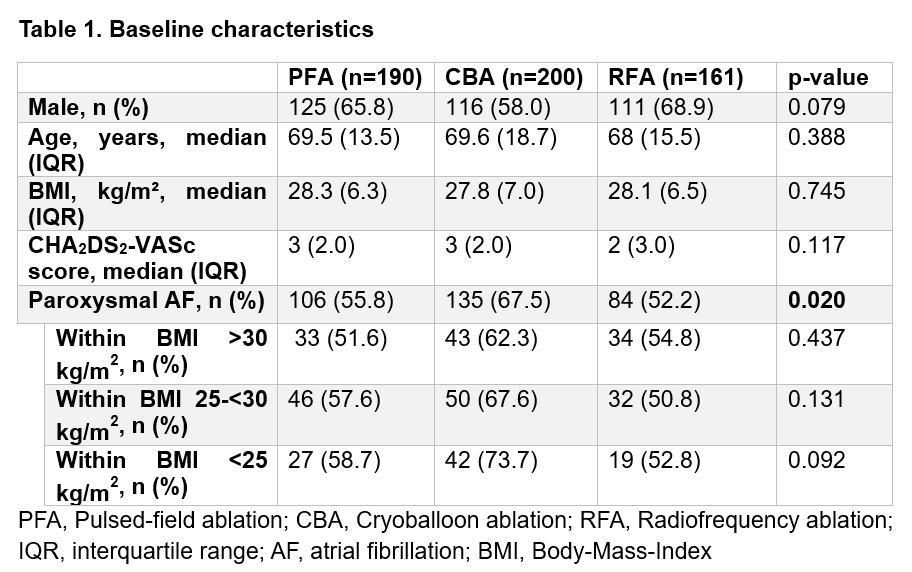
A total of 551 patients were included (PFA: n=190, CBA: n=200, RFA: n=161). Baseline characteristics were comparable except for a higher proportion of paroxysmal AF in the CBA group (p=0.02), while type of AF was balanced within the BMI subgroups (Table1).
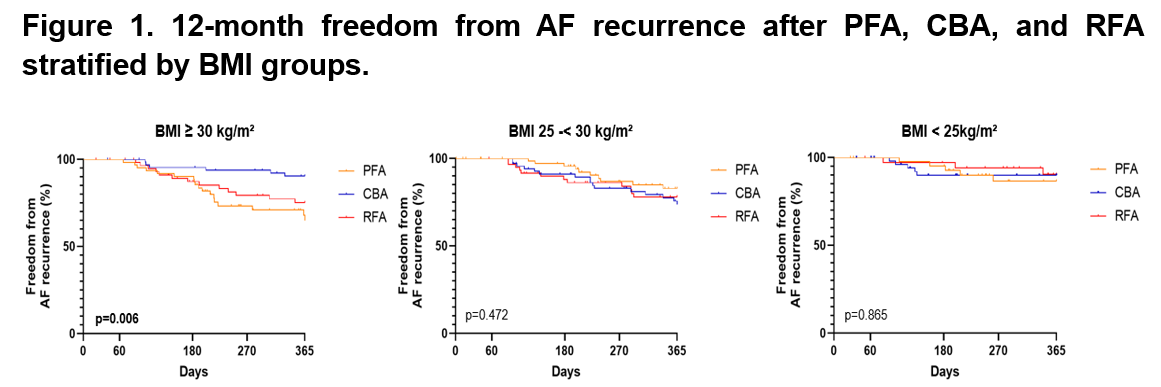
In the overall cohort, 12-month AF-free survival was comparable across PVI modalities (PFA 81.8%, CBA 85.9%, RFA 82.3%, p=0.33). However, among obese patients, freedom from AF was significantly different (p=0.006, Figure 1), with the highest rate observed in the CBA group (91.2%) when compared to RFA (78.3%) or PFA (71.0%). In overweight or normal-weight patients, the clinical outcome was not different between PVI modalities (p=n.s., Figure 1).
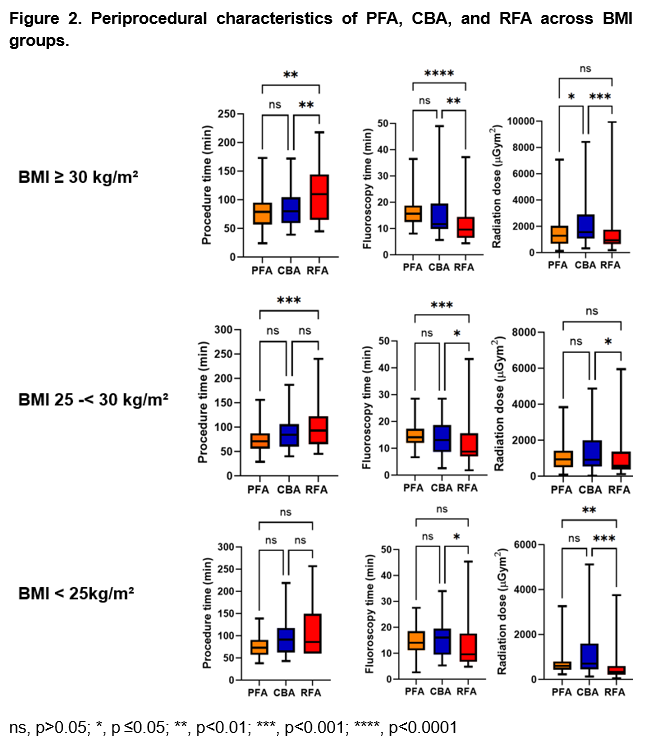
In the obese patient cohort, PFA and CBA were associated with significantly shorter procedure times when compared to RFA, with a trend toward shortest procedure times achieved with PFA irrespective of BMI (Figure 2). In contrast, fluoroscopy time was consistently lowest with RFA across all BMI subgroups, while PFA and CBA showed comparable values across BMI strata. This translated into the lowest radiation dose observed with RFA irrespective of BMI. PFA was associated with a lower radiation dose when compared to CBA in the obese patient cohort (Figure 2). With respect to complications, we observed comparable complication rates in the overall cohort (PFA 5,26%, CBA 5,5 %, RFA 5,59%, p=0.99) and also BMI subgroups (p=n.s.).
Conclusion
Overall, PFA, CBA, and RFA demonstrated comparable 12-month freedom from AF recurrence. In obese patients, CBA, was associated with a higher AF-free survival. PFA showed the shortest procedure duration compared to all other PVI modalities independent of BMI. While RFA in general was associated with lowest radiation exposure, in the obese patient subgroup, PFA-PVI was achieved with comparatively low radiation dose, as opposed to CBA. These results provide insights into the role of distinct PVI modalities related to BMI emphasizing the need to consider BMI when tailoring the optimal ablation strategy to the patient and operator.