Patient presentation
Transcatheter edge-to-edge repair (T-TEER) has emerged as an effective and safe therapy for severe symptomatic tricuspid regurgitation (TR). Nevertheless, procedural complications and technical limitations can occasionally lead to failure, necessitating alternative transcatheter solutions. We present the case of a 77-year old woman referred for T-TEER due to severe TR and New York Heart Association (NYHA) functional class III symptoms with peripheral edema and dyspnoe on mild exertion. Echocardiography revealed a Hahn type IIIB quadricuspid valve with preserved biventricular function.
Initial work up
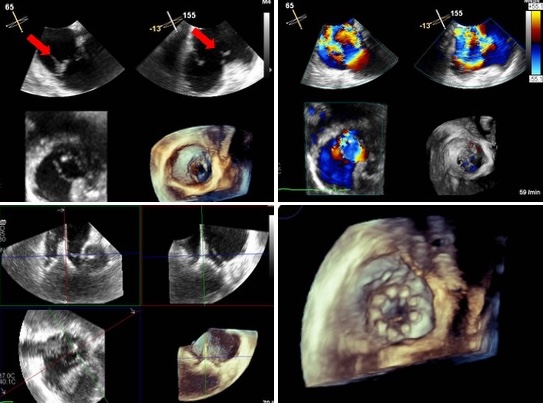
During the TEER procedure, restricted maneuverability of the delivery system due to insufficient height and entanglement within the anterior subvalvular apparatus resulted in partial rupture of the anterior papillary muscle with flail leaflet and consecutive torrential TR. The procedure was aborted, and subsequent multimodality imaging with cardiac computed tomography and echocardiography was performed immediately. Imaging confirmed feasibility for both homotopic and heterotopic TTVR. In light of the patient's hemodynamic and functional stability, as well as patient preference, the Heart Team opted for a staged, homotopic TTVR.
Diagnosis and management
Following a brief period of rehabilitation and clinical stabilization, a planned homotopic TTVR was successfully performed using a 48-mm self-expanding bioprosthesis via left femoral venous access in order to gain more height for maneuverability. Controlled pharmacological asystole with intravenous adenosine facilitated precise anchoring and optimal leaflet engagement during atrial expansion and final release of the prosthesis.
Follow-up
Post-implantation echocardiography demonstrated complete TR elimination, preserved right ventricular function, and no gradient across the prosthesis. No conductions disturbances were detected during postprocedural monitoring. The patient experienced substantial symptomatic improvement and was discharged home in good condition four days later.
Conclusions
This case highlights the feasibility of timely rescue TTVR following failed T-TEER, demonstrating how prompt multidisciplinary reassessment and tailored imaging can convert procedural complication into a durable success.