Background
Randomized trials have shown a non-inferiority for two pulsed field ablation (PFA) systems (PulseSelect™ Medtronic, PFA-P; FARAPULSE™ Boston Scientific, PFA-F) compared to thermal pulmonary vein isolation (PVI) modalities. Comparative real-world data on the experiences with these two ablation systems is scarce. Aim of our study was to assess the feasibility of implementing PFA-P in a PFA-F experienced center.
Methods
This single center retrospective study included 150 patients who underwent first-PVI with PFA-P and PFA-F between Juli 2024 and September 2025, performed by three experienced electrophysiologists, who have performed over 200 PFA-F PVIs each. Procedural characteristics and myocardial biomarkers and short term outcome post ablation were analyzed.
Results
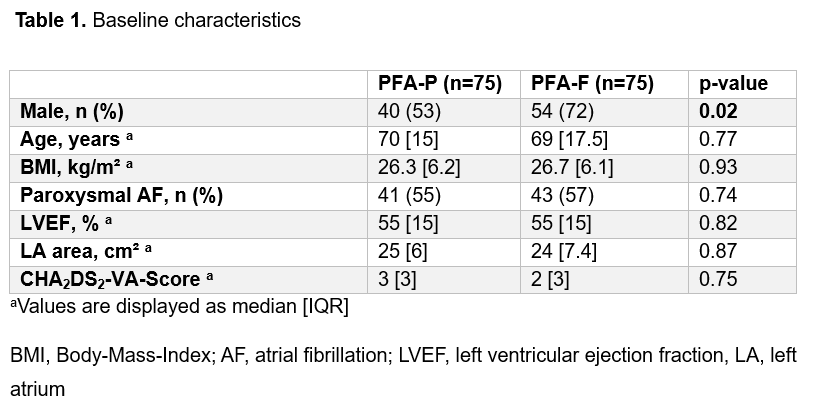
The study included predominantly male patients with a median age of 69.5 years (Table 1). Complete PVI was achieved in 98% and 100% with isolation after eight manufacturer-recommended impulses per vein in 82.7% and 77.3% of patients (p=0.42), for PFA-P and PFA-F respectively.
Fluoroscopy time was significantly higher in the PFA-P group (14.3 [4.2] vs. 11.9 [7.9] min, p=0.009), while skin-to-skin time (45 vs. 44.5 min, p=0.36) and radiation dose (12.1 vs. 11.0 Gy*cm2, p=0.30) were comparable for PFA-P and PFA-F, respectively. Both groups required comparable dosage of propofol (300 vs. 295 mg, PFA-P and PFA-F respectively, p=0.52) and fentanyl (0.1 mg in both groups; p=0.32). The periprocedural complication rate was similar within the groups (4% vs. 5.3%), no major complication was observed, while minor vascular complications, aspiration, coronary spasm and a strong vagal reaction were experienced.
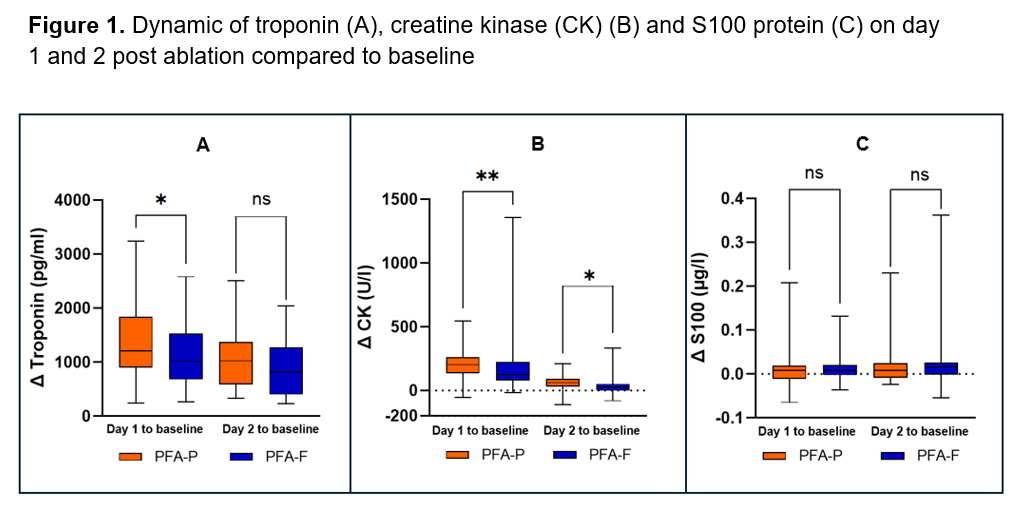
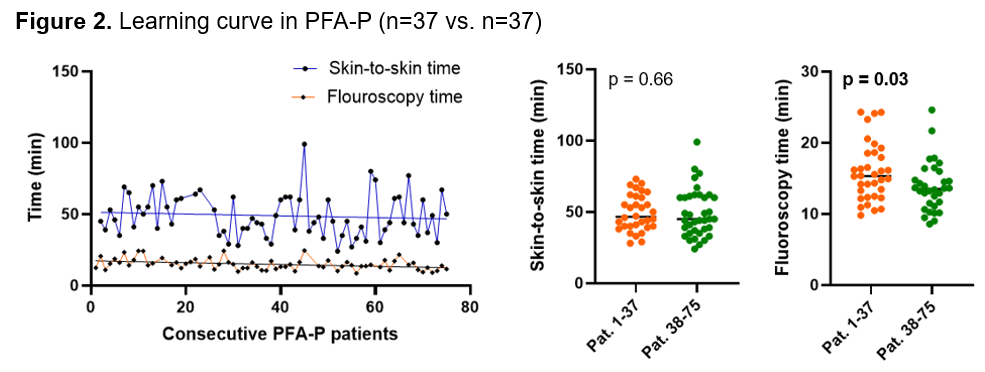
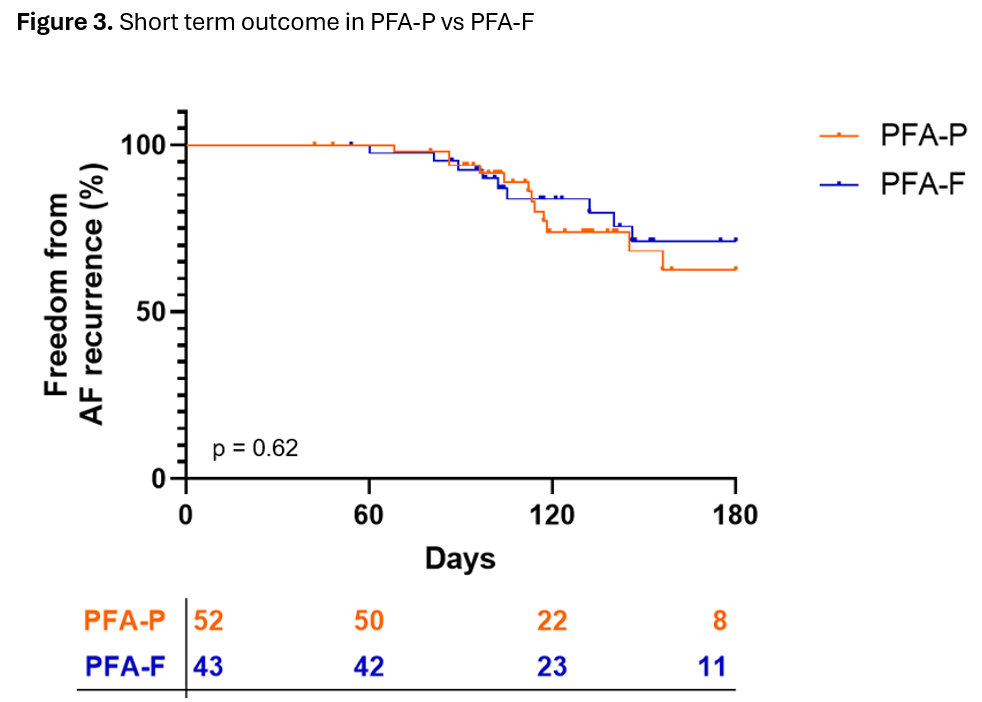
On day 1, PFA-P was associated with greater increases in troponin (Δ 1212 [930] vs. 1014 [809] pg/mL, p=0.04) and CK levels (Δ 203 [118] vs. 127 [141] U/L, p=0.006) compared to PFA-F. On day 2, both markers remained higher after PFA-P (troponin: Δ 1026 vs. 821 pg/mL, p = 0.06; CK: Δ 61 vs. 26 U/L, p=0.01), with the troponin difference not reaching statistical significance. Δ S100 protein levels were comparable between groups on day 1 (p=0.74) and day 2 (p=0.40) post ablation (Figure 1). In a subanalysis of the PFA-P cohort for a potential learning curve (first vs. last 37 cases), fluoroscopy time decreased significantly (15.3 vs. 13.5 min), while skin-to-skin time remained unchanged (46.5 vs. 45 min; Figure 2). Short term follow-up (117 [57] days) revealed no difference in AF recurrence (p=0.62) (Figure 3).
Conclusion
This study demonstrates that PFA-P can be safely and effectively implemented in a PFA-F experienced center. Higher postprocedural troponin and CK levels after PFA-P suggest a greater extent of myocardial injury. Short-term follow-up shows similar rate for AF recurrence. These results suggest PFA-P being a valid and equivalent alternative as a PVI-PFA-single-shot device compared to PFA-F. Further studies with larger patient numbers, re-do analysis with 3-D mapping, and long-term follow-up are warranted to elucidate the clinical relevance of these findings.