Background:Early risk stratification in acute pulmonary embolism (PE) remains challenging, particularly when differentiating intermediate-high from hogh-risk patients per ESC 2019 criteria. This study aimed to identify independent mortality predictors and to derive the Pulmonary Embolism-Hemodynamic Instability Risk Score (PEHIR).
Methods:A prospective cohort of 499 patients with intermediate-high (n = 267) or high-risk PE (n = 135) was analyzed. Clinical, hemodynamic, laboratory, and imaging parameters were compared. Independent mortality predictors were identified using multivariable logistic regression, and a bedside scoring system (PEHIR) was derived.
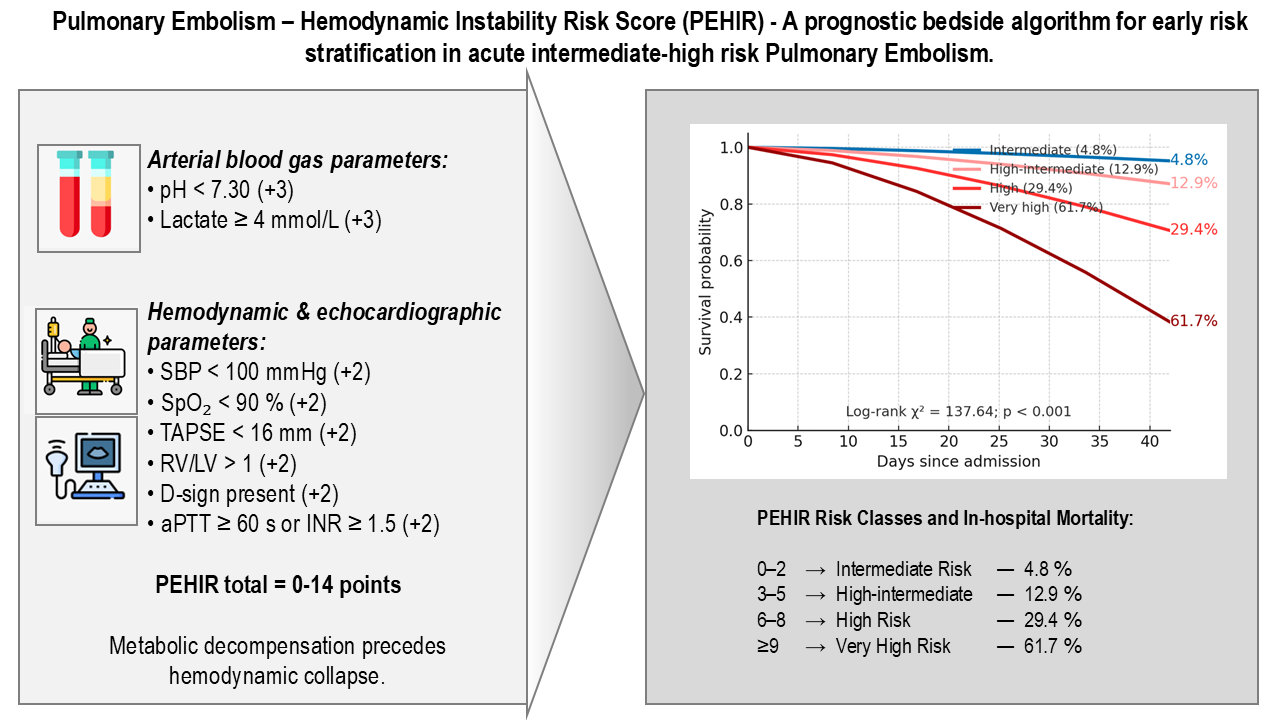
Results:High-risk PE patients had lower systolic blood pressure (108 ± 45 vs. 130 ± 28 mmHg, p<0.01), lower arterial pH (7.21 ± 0.24 vs. 7.41 ± 0.07, p<0.001), higher lactate (7.8 ± 8.2 vs. 3.1 ± 15.0 mmol/L, p<0.001), and more frequent RV dysfunction (TAPSE 15.6 ± 4.9 vs. 18.4 ± 4.8 mm, p<0.01). Catecholamine use (84.5% vs. 13.7%, p<0.001), intubation (77.5% vs. 10.3%, p<0.001), and in-hospital mortality (62% vs. 10%, p<0.001) were markedly higher in the high-risk group. Independent mortality predictors included arterial pH < 7.30, lactate ≥ 4 mmol/L, systolic BP < 100 mmHg, SpO₂ < 90%, TAPSE < 16 mm, RV/LV > 1, D-sign, and coagulopathy (AUC = 0.93). The derived PEHIR Score (0–14 points) showed excellent discrimination and calibration.
Conclusion:High-risk PE is associated with profound hemodynamic and metabolic compromise and increased mortality. The PEHIR model enables accurate early mortality prediction and may enhance risk assessment as proposed by the ESC 2019 Guidelines, supporting more individualized treatment strategies.
Graphical Abstract: