Background: Consecutive left atrial tachycardia (cLAT) are commonly occurring after catheter ablation (CA) for atrial fibrillation, particularly after additional left atrial lesions beyond pulmonary vein isolation (PVI). Data on cLAT after previous ablation are still limited.
As CA procedures are expanding and involve larger-footprint systems, the occurrence of cLAT may increase. Consequently, understanding ablation success of cLAT has become an area of growing clinical relevance.
Aim: To assess durability of linear lesions for treatment of cLAT, predictors of re-ablation after CA of cLAT and periprocedural safety outcomes in a large real-world cohort.
Methods: Consecutive patients treated for cLAT with radiofrequency CA (RFA) between 2017 and 2025 were retrospectively analyzed. Baseline characteristics and periprocedural complications were identified using ICD-10 and OPS codes. Patients admitted for re-ablation after cLAT-procedure were assessed for reconduction of ablation lines and predictors for recurrence.
Results: A total of 484 patients were included [median age of 72 (IQR 65-77), 292/484 (60%) male, arterial hypertension 298/484 (62%), heart failure 101/484 (21%), diabetes 59/484 (12%), coronary artery disease 113/484 (23%), prior stroke 8/484 (1.7%) and peripheral artery disease 5/484 (1%)]. Applied lesion sets by identified cLAT mechanisms consisted of: anterior line [294/484 (61%)], roof line [144/484 (30%)], focal ablation [136/484 (28%)] and a mitral isthmus line (MIG) [104/484 (22%)]. To achieve complete MIG block in 54% (56/104) an endo- and epicardial CA approach was necessary.
Overall complication rates revealed groin bleeding/hematoma in 41/484 (8.5%) and pericardial tamponade in 6/484 (1.2%) patients, requiring surgical treatment in one case. In 2/484 (0.4%) patients transitory ischemic attack occurred, in 7/484 (1.4%) pacemaker implantation due to sinus node dysfunction or high-degree AV block was necessary. There were no periprocedural deaths.
After the cLAT procedure, 113/484 (23%) patients underwent repeat ablation mostly for recurrence of AT 72% (81/113). In these 113 repeat ablation procedures a total of 133 ablation lines were evaluated.
Reconnection was seen in 61/133 (46%) of the linear lesions, including reconnection of the anterior line in 35/73 (48%), roof line 12/32 (38%) and MIG 14/28 (50%). There was no significant difference in durability between these lesions.
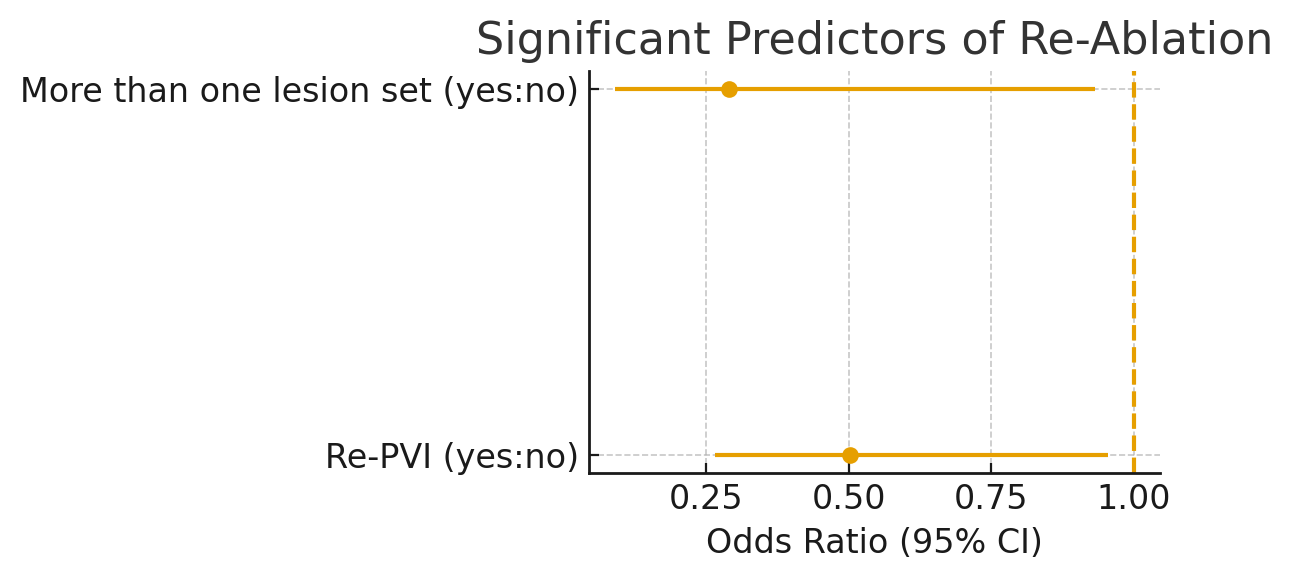
Multiple lesion sets and re-PVI during the cLAT procedure significantly reduced the risk for recurrence (odds ratio (OR) 0.290; confidence interval (CI) 0.09–0.932; p = 0.038), (OR 0.503, CI 0.265-0.954 p=0.035).
Conclusion: In patients admitted with cLAT CA is safe and effective with favorable outcome. However, previous blocked linear lesions lack long term durability. New catheter designs and energy modalities may improve durability and therefore outcomes after CA for cLAT.