Background: Oesophageal fistula (OF) represents a rare but dreadful complication of atrial fibrillation (AF) catheter ablation. The POTTER-AF study reported its incidence, management, and outcomes. However, the temporal evolution of management strategies and patient outcomes has not been evaluated to date.
Aims: This POTTER-AF sub-study aimed to assess the time course of OF formation and management to determine whether increasing awareness and preventive measures have reduced mortality and sequelae rates over time.
Methods: The international multicentre POTTER-AF registry included 138 patients with OF among 553,729 AF ablation procedures. In 116 (84%) patients, the ablation date was available; the remaining were excluded from this sub-study. Based on the procedure date, patients were divided into three time periods (T1: 2004–08/2014, n=39; T2: 08/2014–04/2018, n=39; T3: 05/2018–10/2022, n=38).
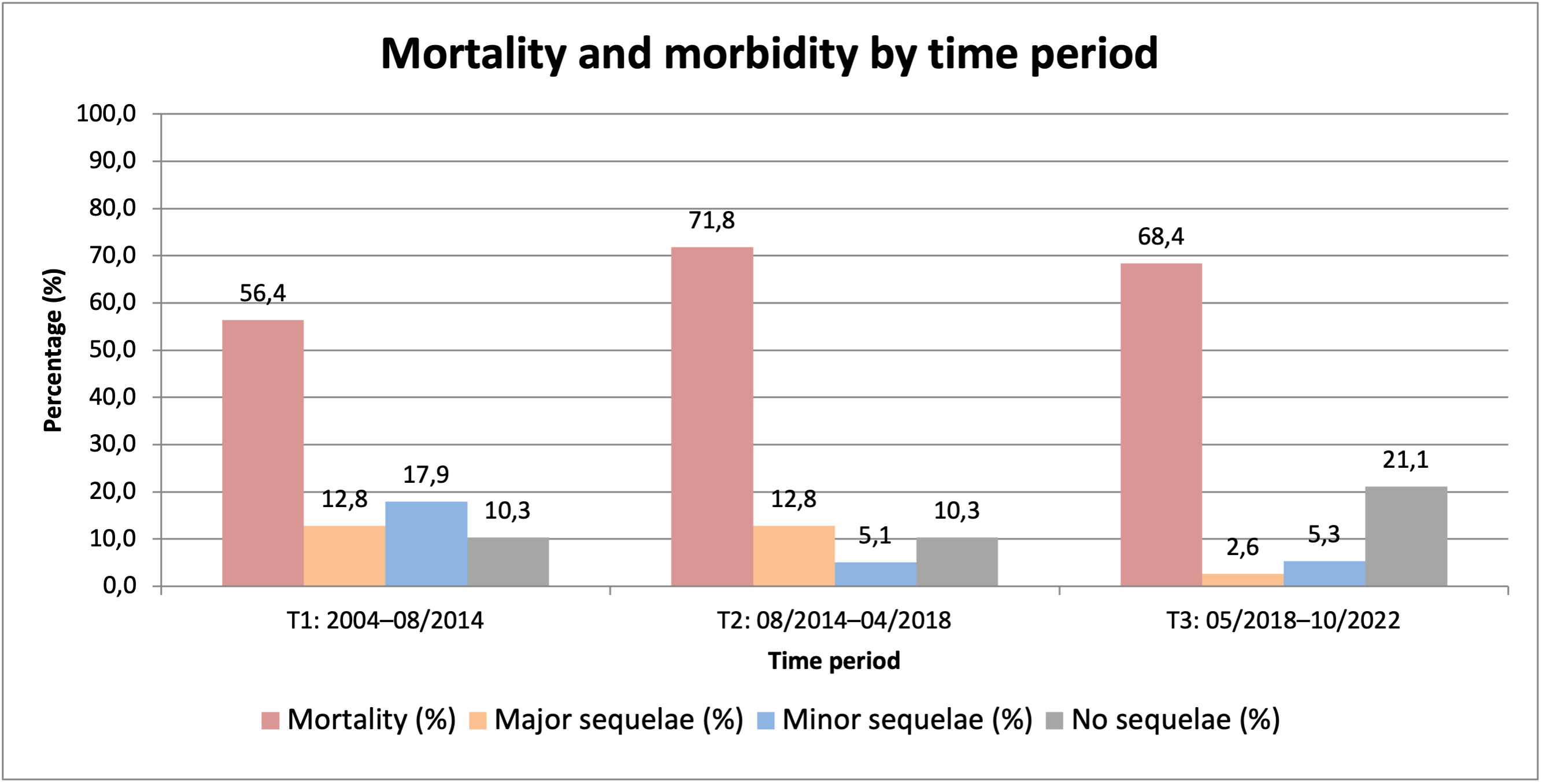
Results: Post-procedural proton pump inhibitors were prescribed in 71.6% of patients (T1: 51.3%, T2: 76.9%, T3: 86.8%; p=0.017), and an oesophageal temperature probe was used in 24.1% (T1: 17.9%, T2: 35.9%, T3: 18.4%; p=0.107). Oesophageal surgery was performed in 39.7% (T1: 28.2%, T2: 46.2%, T3: 44.7%; p=0.198), direct endoscopic treatment in 19.0% (T1: 17.9%, T2: 23.1%, T3: 15.8%; p=0.703), and conservative treatment in 32.8% (T1: 43.6%, T2: 17.9%, T3: 36.8%; p=0.044). Overall mortality was 65.5% (T1: 56.4%, T2: 71.8%, T3: 68.4%; p=0.324). The rate of major sequelae was 9.4% (T1: 12.8%, T2: 12.8%, T3: 2.6%; p=0.213), minor sequelae 9.4% (T1: 17.9%, T2: 5.1%, T3: 5.3%; p=0.086), and no sequelae 13.4% (T1: 10.3%, T2: 10.3%, T3: 21.1%; p=0.286).
Conclusions: Despite growing experience and wider use of preventive measures such as proton pump inhibitors, mortality and sequelae rates remain high in patients developing oesophageal fistula after AF ablation.