A 25-year-old male presented with a six-month history of acute left-sided chest pain, exertional dyspnoea and moderate tachycardia. Initial assessment included laboratory testing, echocardiography, chest X-ray, coronary angiogram, and cardiac magnetic resonance imaging (CMR). Due to ST-segment elevations in the inferolateral leads, distinct pericardial effusion and slightly elevated C-reactive protein and cardiac enzymes a peri-myocarditis was diagnosed and treated with colchicine and ibuprofen. This resulted in transient clinical reconvalescence. Following cessation of medical therapy three months later, re-evaluation due to symptom relapse revealed no additional findings.
After sixth months, the patient presented with complaints of left sided chest pain and exertional dyspnoea, additionally to our clinic. He also reported position-dependent resting dyspnoea. On echocardiography he showed an unclear extracardiac mass with right-ventricular compression and functional right-ventricular outflow tract obstruction, but without features of restrictive physiology. Chest X-ray, computer tomography (CT) and CMR revealed a massive mediastinal bulk tumor causing complete encasement of the aorta and pulmonary artery, with no evident invasion of the peri- or myocardium (Figure). A CT-guided puncture within 24 hours resulted in the diagnosis of synovial sarcoma. Staging investigation revealed no further metastatic disease and emergency radiochemotherapy was initiated, achieving partial remission and resolution of symptoms after one cycle.
Conclusion: Even though thoracic synovial sarcoma remains a very uncommon differential diagnosis of chest pain and exertional dyspnoea, this case impressively illustrates the critical importance of thorough re-evaluation in patients with recurrent chest pain, even in case of an conclusive, established diagnosis.
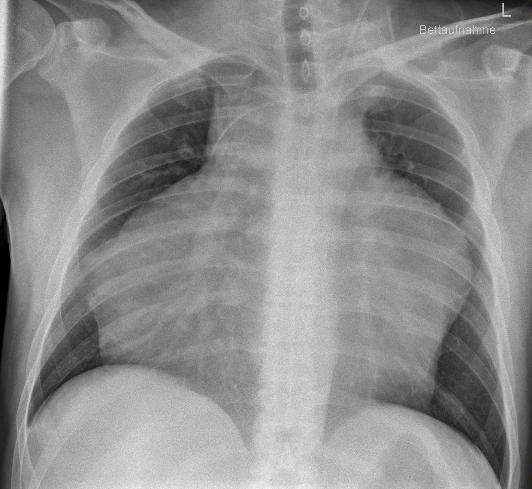
Figure: pa chest X-ray with central venous catheter and mediastinal bulk tumor.



