Introduction: Previous studies have shown that women with acute myocardial infarctions have higher mortality rates compared to men, which is often attributed to atypical symptoms and late presentations. In many studies part of the higher mortality can be attributed to a higher age, since women in studies are often on average older than men during the index event. Aim of the present study was to show, how mortality rates were affected by age and in which age group the disadvantage for women with STEMI was most pronounced.
Methods: All patients, admitted with STEMI to a large German PCI center between 2006 and 2022 were analyzed. Patients were stratified by age into five groups: ≤50 yrs. , 51-60 yrs. , 61-70 yrs. , 71-80 yrs. , >80 yrs. Mortality data was presented in a univariate model and in a multivariate comparison with a Cox regression model.
Results: Of a total of 12093 STEMI-patients, 3343 (27.6%) were women, which were on average 7.6 years older during the index event (69.8±13 yrs. in women vs. 62.2±12 yrs. in men) and were more likely to present without chest pain (11.9% vs. 8.5%, p<0.01). 30-day-mortality rates were higher in women compared to men : 15.3% vs. 9.6 %, p<0.01 and within 5 years: 33.8% vs. 22.2% in men (p<0.01). When adjusting for confounders (age, multivessel disease, PCI success, peak CK) the worse prognosis for women remained at 30 days (HR 1.38, 95% CI 1.2-1.6, p<0.01). However, when stratifying by age group, the higher mortality rates for women only remained significant in very young and in old patients with STEMI, while for all patients between 51 and 80 yrs. of age (71.6% of the cohort) no impact of sex on short and long-term-outcome could be shown in a univariate model (figure, left side) and in a Cox-regression-model (figure, right side).
Figure: Age stratified analysis of impact of sex on 30 day mortality
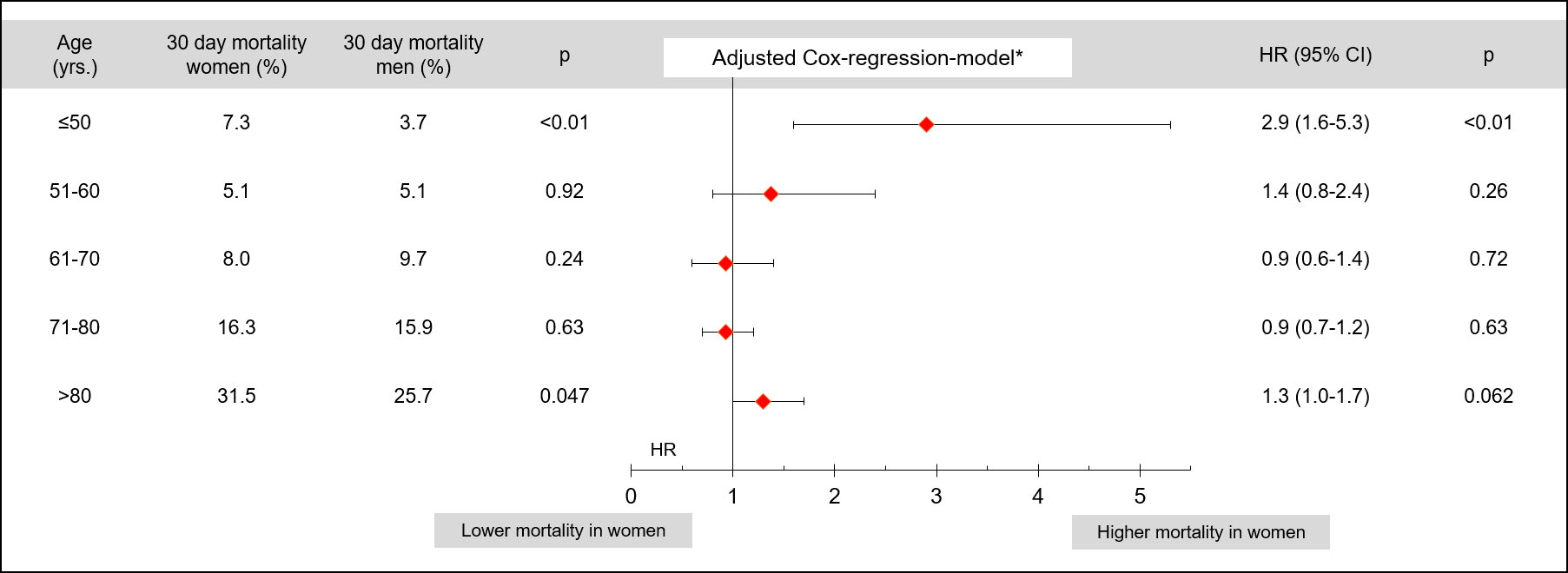
*HR for female sex on mortality adjusted for age, multivessel disease, PCI success, peak CK (Cox regression-model)
Conclusions: This analysis of patients with STEMI shows, that while for the entire cohort female sex was associated with a worse short and long-term prognosis, age stratification revealed that this disadvantage was only evident in very young and old STEMI-patients. For STEMI-patients aged between 51 and 80, which constituted more than 2/3 of the entire cohort, female sex did not impact mortality. Further studies are needed to elucidate the reasons for these age-dependent mortality differences between women and men with STEMI.



