Objective
Catheter ablation for paroxysmal supraventricular tachycardias (PSVTs) is highly effective but entails variable resource demands and procedural risks across arrhythmia subtypes. This study aims to provide an in-depth analysis of patient demographics and comorbidities, acute peri-procedural outcomes, and ablation strategies across distinct PSVT subtypes.
Methods
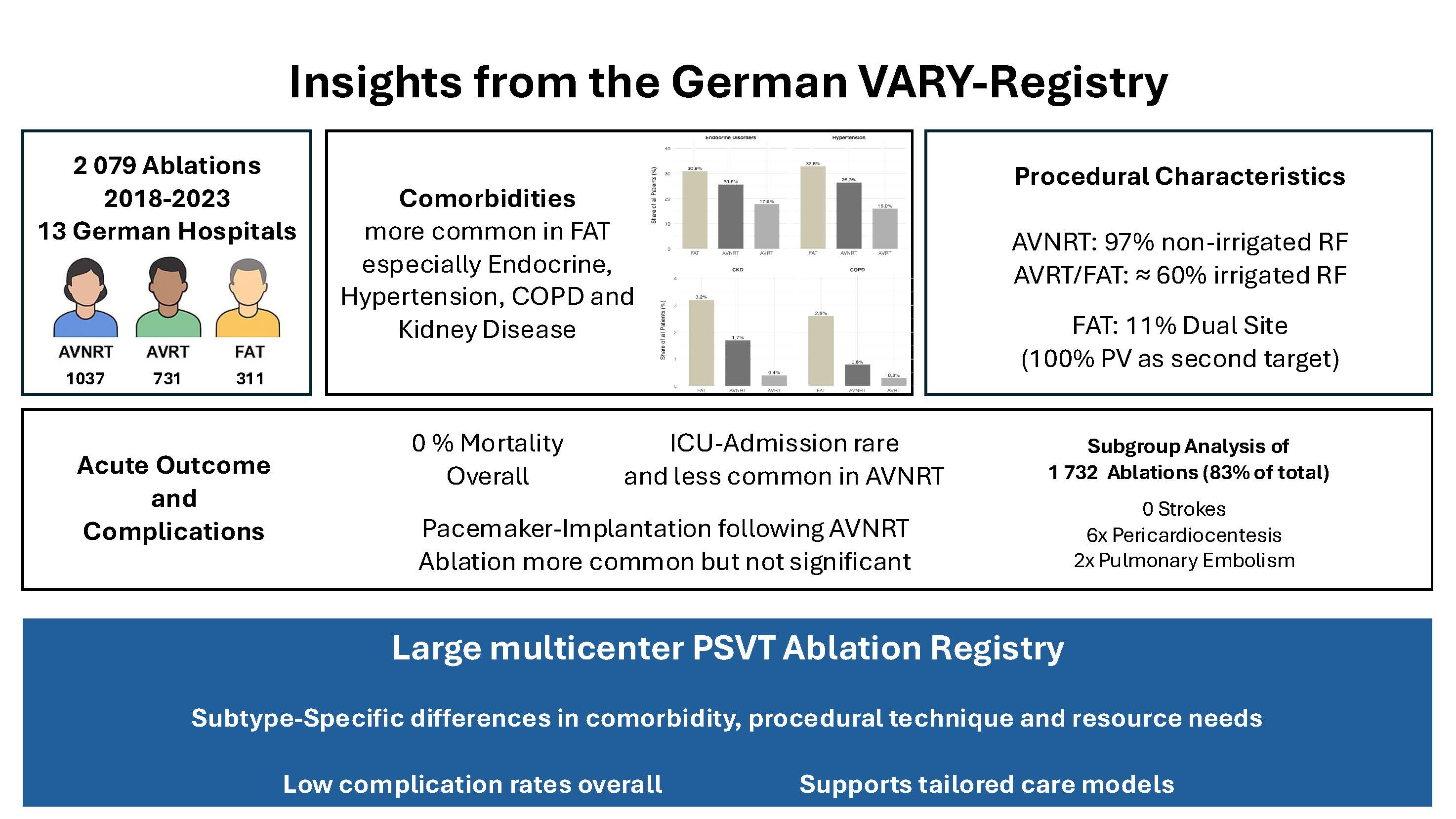
We retrospectively analyzed 2,079 inpatient PSVT ablations, including 1,037 atrioventricular nodal reentrant tachycardia (AVNRT), 731 atrioventricular reentrant tachycardia (AVRT), and 311 focal atrial tachycardia from the left atrium (FAT) procedures performed at 13 German hospitals from 2018 to 2023. We evaluated demographics, comorbidities, hospital-specific parameters, complications, and procedural parameters. Continuous variables are presented as mean ± SD and median; categorical variables as counts and percentages. We compared subgroups using Pearson’s chi-squared test and the Kruskal–Wallis test, with p < 0.05 denoting significance. Additional rare complication data (pericardiocentesis, pulmonary embolism, stroke, major vascular injury) were available for a predefined subgroup of 1 732 cases (83.3 % of the cohort).
Results
No periprocedural deaths were reported. ICU admission rates differed by subtype (AVNRT 2.7%, FAT 4.5%, AVRT 4.9%; p = 0.04), while pacemaker implantation occurred in 1.3 % of AVNRT, 0.6% of FAT, and 0.4% of AVRT cases (p = 0.15). Comorbidity profiles varied markedly: hypertension and endocrine disorders were most prevalent in AVNRT and FAT compared with AVRT (up to 32.8% and 30.9%; both p < 0.001), whereas COPD (2.6%, p = 0.0011) and chronic kidney disease (3.2%, p = 0.0019) clustered in FAT. Procedurally, all AVNRT ablations used RF energy (96.7% non-irrigated), whereas in FAT and AVRT irrigated RF was more often used (69.8% and 65.7%, respectively; p < 0.01). FAT ablations targeted one focus in 88.7% of cases and two in 11.3%, with the pulmonary veins involved in all dual-site procedures.
In the subgroup with extended complication data, pericardiocentesis occurred in 3 AVNRT and 3 AVRT cases (p = 0.49), pulmonary embolism in 2 AVNRT cases (p = 0.40), and major vascular complications requiring intervention in 1 AVNRT case. There were no reported strokes or tamponades either periprocedural or within the hospital stay due to ablation.
Conclusion
AVNRT, AVRT, and FAT differ in ICU utilization, pacing requirements, comorbidity burden, and ablation strategies. Subgroup analysis of rare events shows overall very low rates of serious complications across all PSVT subtypes. These findings support targeted risk stratification, tailored resource allocation, and optimization of procedural planning.



