A 64-year-old man presented to the emergency department of Helios Hospital Erfurt with fever and dyspnea. He had a four-month history of chronic osteomyelitis with abscess formation in the right thumb caused by Methicillin-sensitive Staphylococcus aureus (MSSA), treated with multiple surgeries and antibiotic regimens.
On admission, he showed fever (39.5 °C), hypoxia, and elevated inflammatory and cardiac markers (CRP 44 mg/l, troponin 733 ng/l, NT-proBNP 1586 ng/l – laboratory test results shown in Table 1). Chest X-ray (Fig. 1) revealed cardiopulmonary overload. Echocardiography demonstrated heart failure with mildly reduced ejection fraction (LVEF 43%) and a circular pericardial effusion.
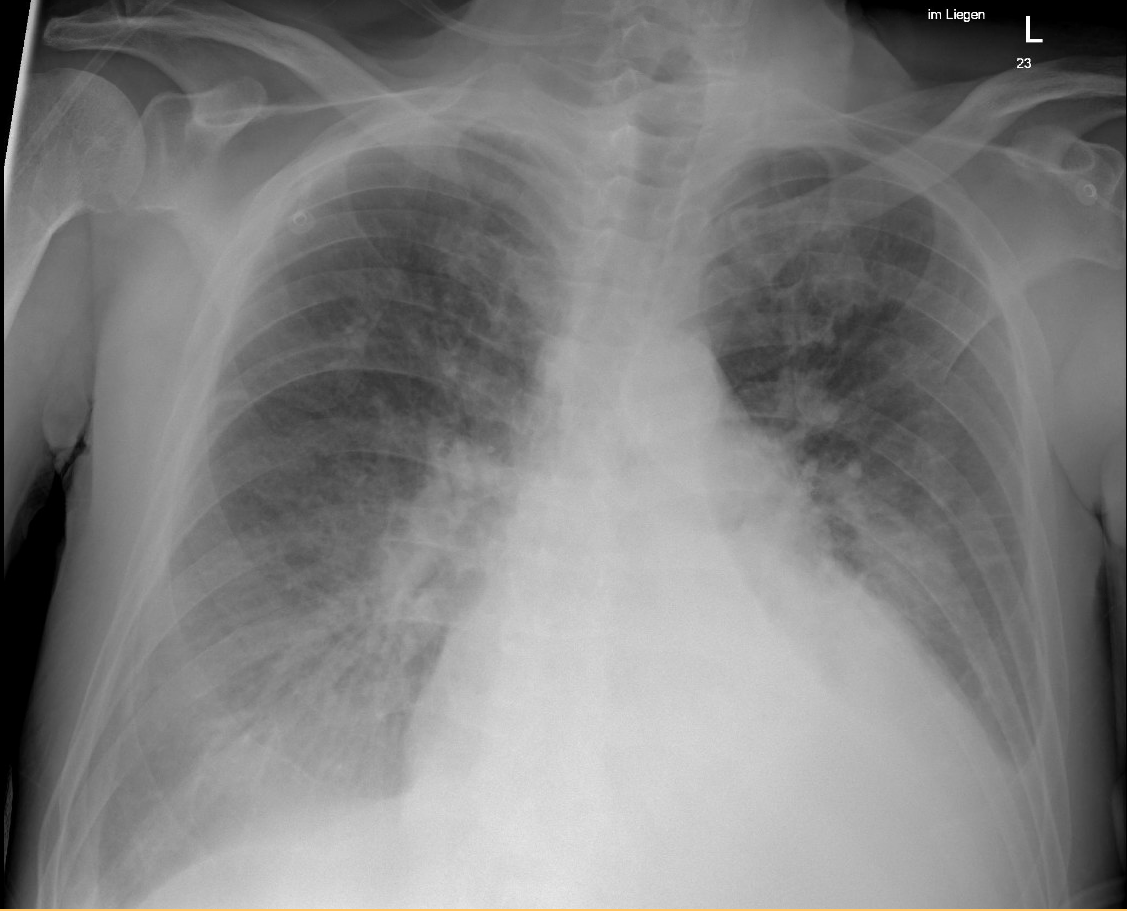
Figure 1.
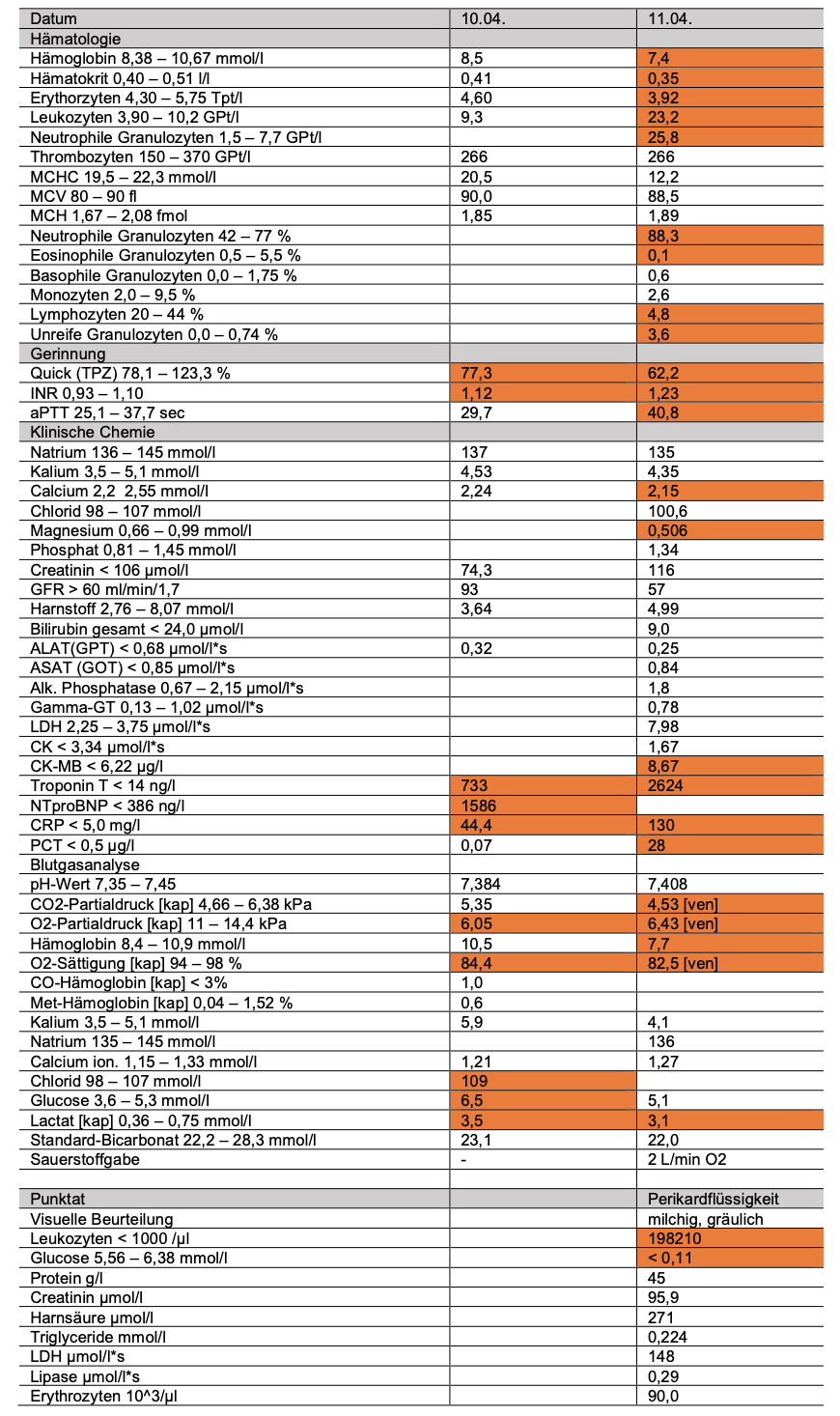
Table 1.
The following day, his condition worsened with sepsis, acute kidney disease, and rising troponin levels. A CT scan confirmed a progressive inflammatory pericardial effusion, suggesting acute purulent pericarditis. Urgent pericardiocentesis was performed, draining 600 ml of thick pus, which led to immediate hemodynamic stabilization.
Microbiological culture of the pericardial fluid identified Proteus mirabilis – a rare cause of pericarditis. The patient received systemic antibiotic therapy (initially piperacillin/tazobactam, then ceftriaxone followed by ciprofloxacin) and local pericardial lavage with heparinized saline and ceftriaxone over several days.

Figure 3: Pericardial fluid still purulent after 5 days of therapy
His clinical condition improved steadily. Follow-up echocardiography showed complete resolution of the effusion but persistent heart failure with reduced ejection fraction (LVEF 40%). The patient’s medical history included rheumatoid arthritis treated with etanercept, suggesting immunosuppression as a predisposing factor. The infection likely originated from prior pleural drainage or spread by continuity.
This case dated before the release of current ESC-guideline on inflammatory myopericardial syndrome (IMPS) which combines new recommendations for the management of myocarditis and pericarditis. Cardiovascular magnetic resonance (CMR) is newly introduced as a main diagnostic tool besides endomyocardial biopsy (Class I), while CT scan is recommended for aetiological diagnosis. In case of purulent pericarditis as in our case an urgent pericardiocentesis or surgical window for drainage of purulent fluid is advised (Class I) independently from haemodynamic status. Besides intravenous antimicrobial therapy there are no recommendations for local antibiotic therapy, intrapericardial fibrinolysis should be considered for complete pericardial drainage and to prevent constriction (Class IIa).



