BackgroundInterventional treatment of tricuspid regurgitation (TR) is a rapidly evolving field, but identifying patients who will derive a mortality benefit remains challenging. The TRI-Score has emerged as the most relevant clinical risk score for predicting mortality after transcatheter tricuspid valve intervention (TTVI), demonstrating better prognostic performance than other scores. While it incorporates key clinical and echocardiographic parameters reflecting systemic congestion and organ function, it does not include invasive right-heart hemodynamics, which may further refine prognostic assessment. Integrating invasive right-heart hemodynamic measures like pulmonary vascular resistance (PVR) may provide a more complete representation of right-sided circulatory load. This study aimed to analyze whether combining the TRI-Score with invasively measured PVR improves prediction of 12-month mortality after TTVI.
MethodsIn this single-center prospective cohort, 118 patients with severe TR (≥3 according to Hahn) underwent either edge-to-edge repair (TriClip 12.7 %, Pascal 68.6 %) or minimal-invasive tricuspid valve replacement (TricValve 15.3, EVOQUE 3.4 %). Both the TRI-Score and PVR were obtained prior to intervention. Patients were followed for 12 months after the procedure. The results of the TRI-score were sorted into low-risk and medium-risk versus high-risk categories. A Kaplan–Meier analysis was applied to illustrate survival rates between TRI-Score risk categories. Receiver-operating-characteristic analyses (ROC) with area-under-the-curve (AUC) calculation were conducted to assess their separate and combined predictive performance for all-cause mortality at 12 months.
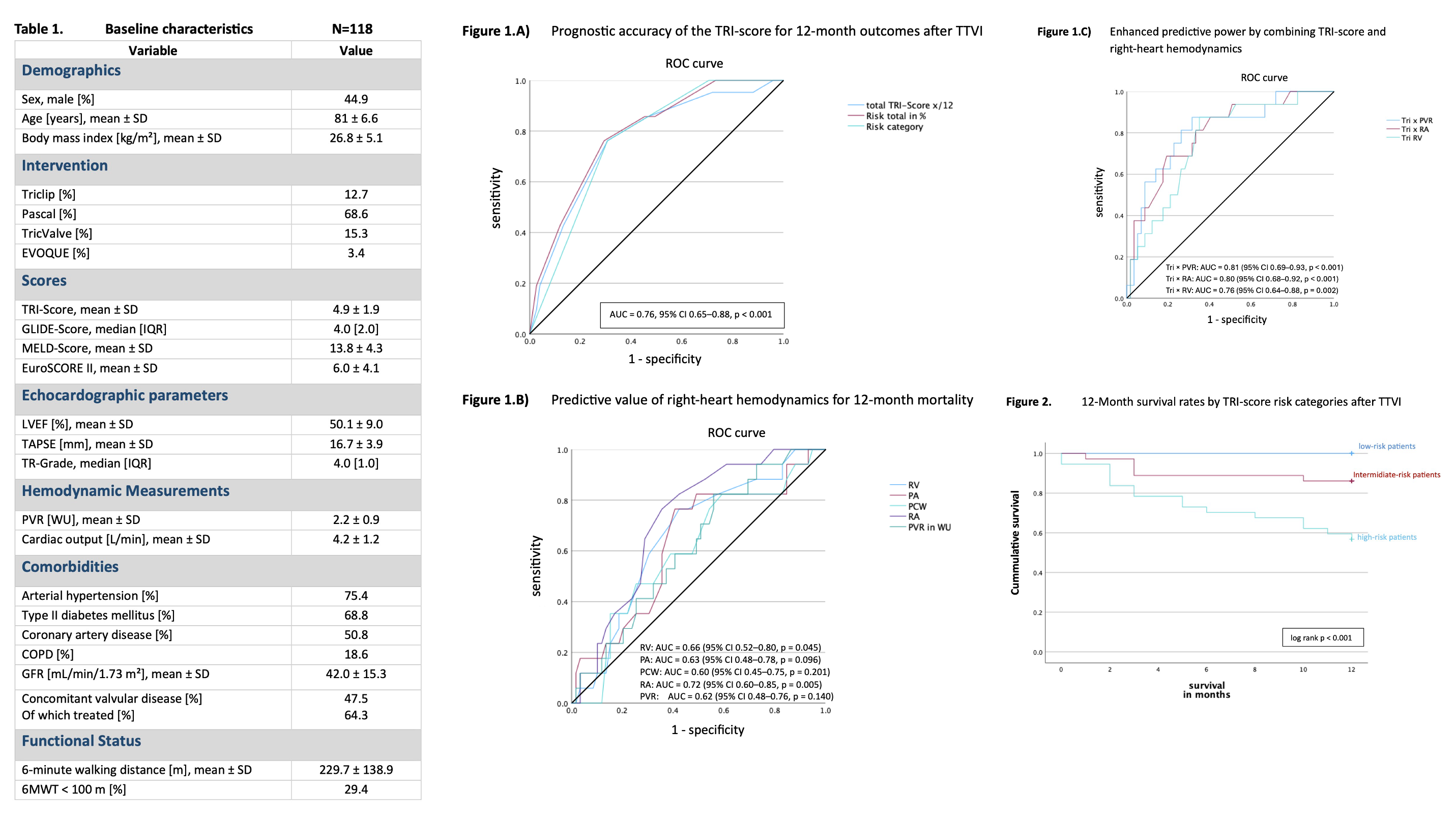
ResultsBaseline characteristics are summarized in Table 1. Within 12 months, mortality occurred in 18.6% of patients. The TRI-Score on its own demonstrated good prognostic discrimination for 1-year mortality (AUC = 0.76, 95% CI 0.65–0.88, p < 0.001) as shown in
Figure 1A. The Kaplan–Meier analysis in
Figure 2 revealed significantly better survival for patients in the low- and intermediate-risk TRI categories (log rank p < 0.001). Among right-heart hemodynamic parameters, both RA and RV pressure showed prognostic relevance for 1-year mortality
(Figure 1B). In contrast, PVR alone demonstrated only modest and statistically insignificant predictive accuracy. However, the combination of the TRI-Score with PVR yielded the highest predictive performance (AUC = 0.81, 95% CI 0.69–0.93, p < 0.001) as shown in
Figure 1C.
ConclusionThe TRI-Score proves to be the most reliable clinical risk score for all-cause mortality assessment after TTVI. The integration of PVR enhances its predictive accuracy.