INTRODUCTION
Coronary-atrial fistulas are rare congenital or acquired anomalies involving abnormal connections between coronary arteries and cardiac chambers. The resulting left-to-right shunt can provoke a coronary steal phenomenon, which in turn may cause myocardial ischemia. They are associated with complications such as arrhythmia, heart failure or endocarditis. Early detection, quantification and timely closure may prevent long-term sequelae. In patients with complex cardiovascular histories, such as Marfan syndrome and prior aortic surgeries, these fistulas can complicate coronary artery disease management. This case illustrates the challenges and outcomes of percutaneous closure in a symptomatic patient with an aneurysmatic right coronary artery (RCA) – to – right atrium (RA) fistula against the background of a Marfan Syndrome.
CASE REPORT
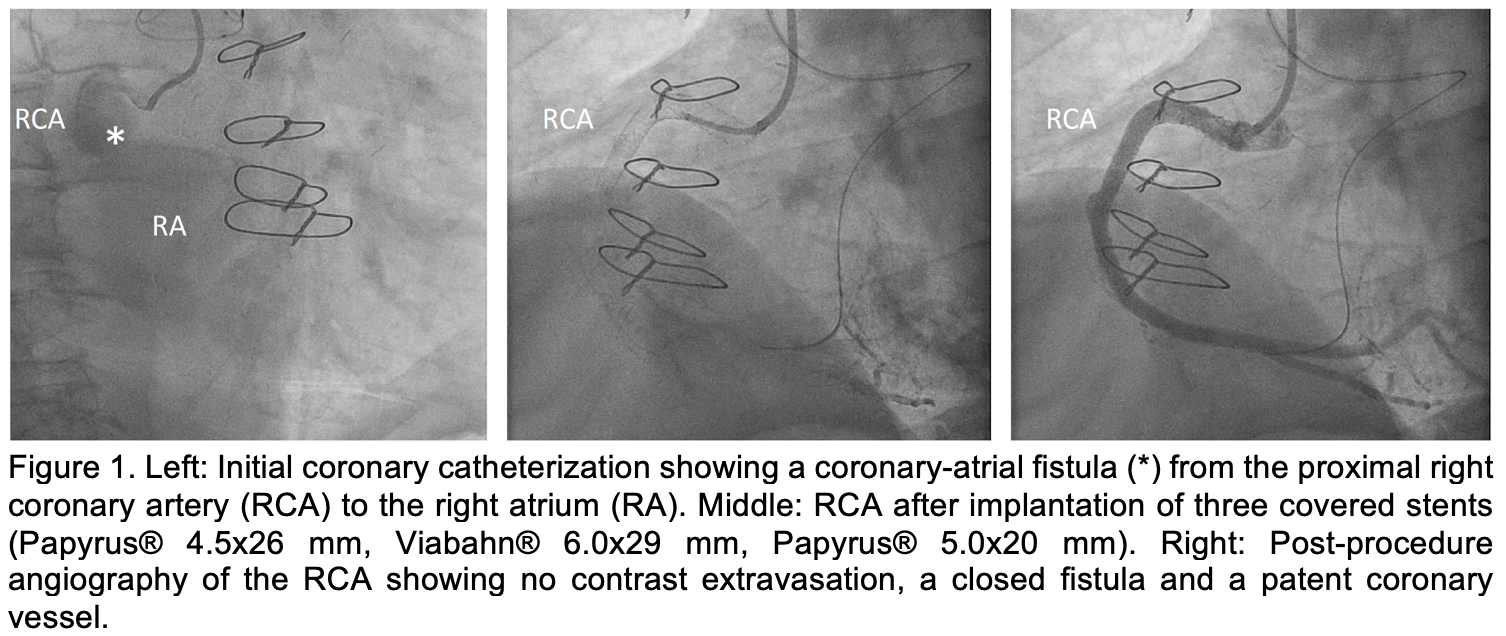
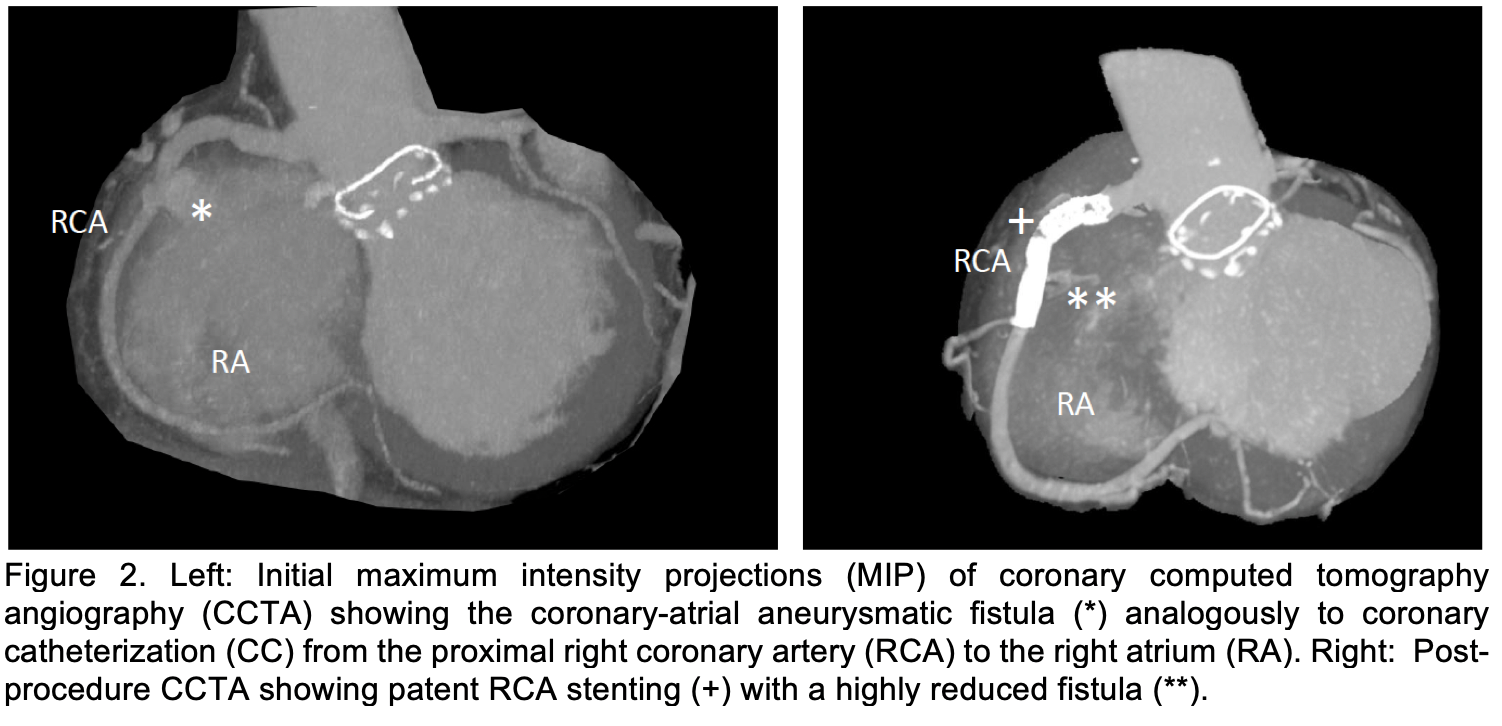
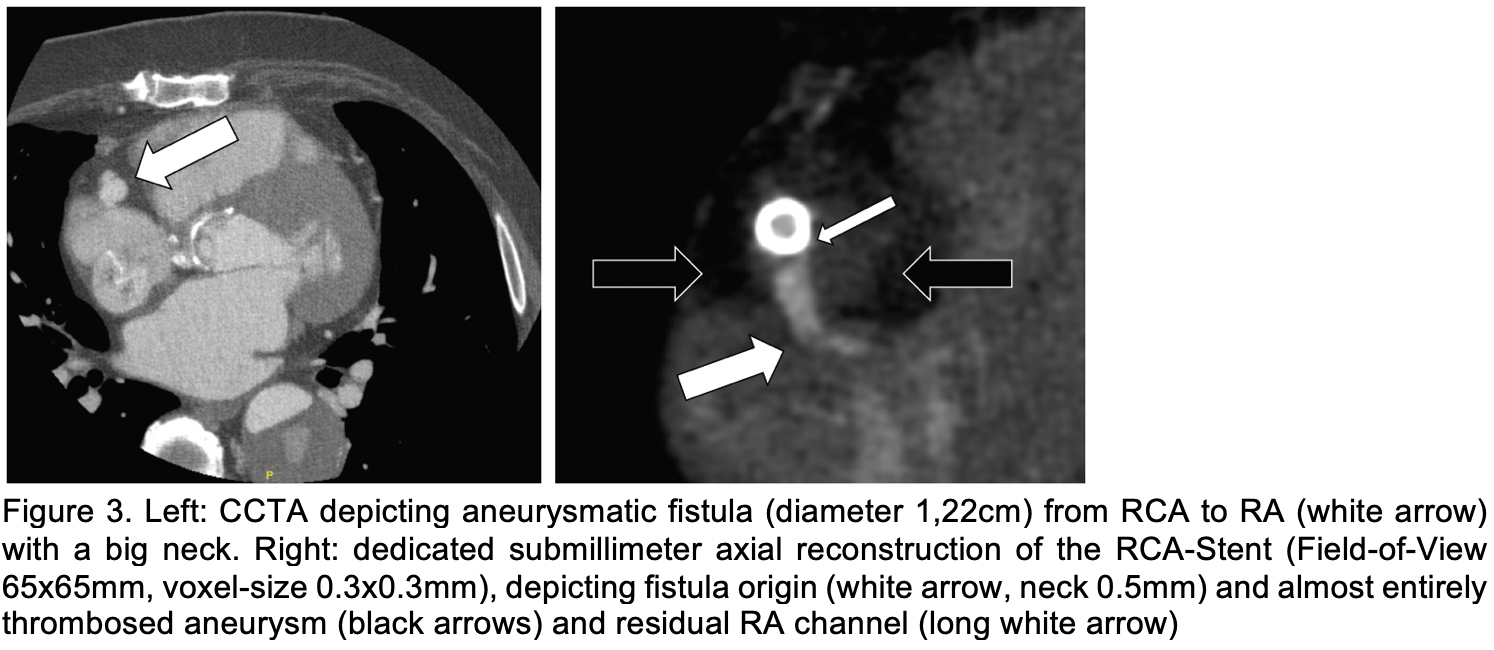
A 61-year-old male with prior ascending aorta, aortic arch and aortic valve replacements (2009 and 2023) in the context of Marfan syndrome, reduced left ventricular ejection fraction (LVEF, 40-45%), and severe mitral valve regurgitation presented with progressive angina, exertional dyspnea, and dizziness lasting for over one year. Coronary catheterization (CC) and coronary computed tomography angiography (CCTA) revealed a coronary-atrial fistula from the proximal right coronary artery (RCA) to the right atrium (RA) with a significant left-to-right shunt (Qp:Qs = 1.4:1) and despite a normal RCA on CCTA, antegrade wire passage from proximal to distal RCA was not possible (Figure 1 and Figure 2). In a second CC session a complex percutaneous intervention was performed, involving retrograde wire passage, snaring, externalization, and implantation of covered stents (Papyrus® 4.5x26 mm, Viabahn® 6.0x29 mm, Papyrus® 5.0x20 mm) to close the fistula and recanalize the RCA (Figure 1). Post-procedure angiography confirmed only minimal contrast extravasation. Dedicated CCTA two days after was performed using deep-learning enhanced iterative reconstruction kernel to minimize metal-artifacts from stents. Furthermore, the contrast medium bolus was tailored to keep the right heart chambers nearly devoid of contrast, thereby enabling visualization of coronary contrast passage. A small residual fistula channel (< 1mm) from the stent (Figure 2 and 3) was visualized. Transthoracic echocardiography (TTE) excluded pericardial effusion and showed an improved LVEF (50-55%). The patient reported improved well-being and was discharged on dual antiplatelet therapy (aspirin and clopidogrel for 6 months), beta-blockers, angiotensin converting enzyme (ACE) inhibitors, diuretics, statins, and thyroid supplementation, with stable renal function and no peri – or postinterventional complications.
CONCLUSION
Image guided percutaneous closure of a coronary-atrial fistula with covered stents is feasible but technically demanding, particularly in patients with concomitant stenosis and high-velocity / flow shunts, where guidewire guidance is increasingly difficult. This case underscores the value of multidisciplinary management in high-risk cardiovascular patients.