Background: Infective endocarditis (IE) requires prolonged antibiotic therapy, often delivered during extended hospital stays. Outpatient antibiotic therapy (OAT) has emerged as a potential alternative in selected patients, but its safety and efficacy are still being defined. The aim of this study was to evaluate the clinical outcomes of patients who received OAT after initial hospitalization, compared to those who received inpatient antibiotic therapy exclusively for left-sided IE.
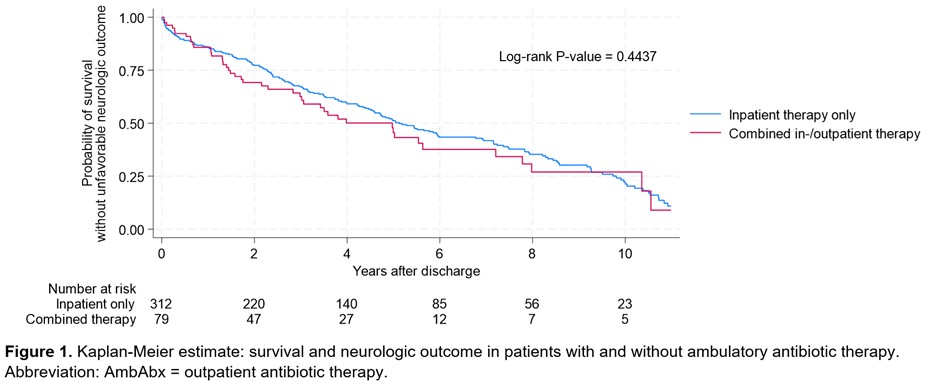
Methods: This observational cohort study included 391 patients with left-sided IE after they were discharged from the hospital. Seventy-nine patients received combined inpatient and outpatient antibiotic therapy, and 312 patients received standard inpatient-only therapy. The primary endpoint was a composite of all-cause mortality and unfavorable neurological function, as assessed at follow-up. We performed Kaplan-Meier analysis and Cox regression modeling, followed by matched subgroup analysis to account for confounding factors.
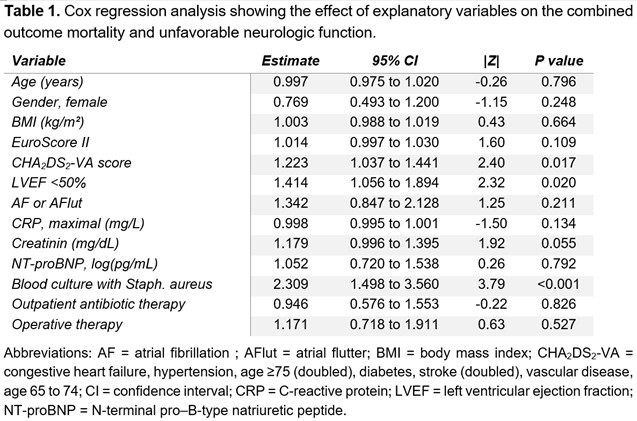
Results: The baseline characteristics differed between the groups. The OAT group had a higher EuroSCORE II (13.0 ± 18.4 vs. 8.2 ± 9.2, pttest = 0.001), fewer abscesses (9% vs. 20%, pchi2 = 0.019), lower NT-proBNP levels (median 2002 pg/mL, interquartile range 456 pg/mL to 4781 pg/mL vs. 2797 pg/mL, 1170 pg/mL to 7033 pg/mL, pranksum = 0.008), and fewer surgical cases (34% vs. 79%, pchi2 < 0.001). Overall, there was no significant difference in the combined endpoint between the OAT group and the standard therapy group after a mean follow-up of 4.1 years (Figure 1). In Cox regression analysis, OAT was not independently associated with the primary endpoint. Significant predictors included the CHA₂DS₂-VA score, the presence of an impaired left ventricular ejection fraction, and a positive blood culture for Staphylococcus aureus (Table 1). After correcting for these confounders in the propensity-matched analysis, the average treatment effect of patients receiving OAT was found to be neutral (coefficient 0.056, 95% confidence interval -0.173 to 0.284).
Conclusion: OAT appears to be a safe and feasible treatment option for select patients with left-sided IE. These findings support the use of OAT in appropriate clinical contexts, especially when careful patient selection and follow-up are ensured.