Introduction: Veno-arterial extracorporeal membrane oxygenation (ECMO) has emerged as a therapy for patients with refractory cardiac arrest. However, the process of weaning from ECMO remains challenging, and optimal strategies are still under investigation. Levosimendan, a calcium-sensitizing agent with inotropic and vasodilatory effects, has shown potential in facilitating ECMO weaning in patients with cardiogenic shock (CS). Yet, data on patients after successful extracorporeal cardiopulmonary resuscitation (ECPR) remain scarce. This retrospective analysis aims to evaluate the efficacy of levosimendan during the ECMO weaning process in patients following ECPR.
Methods: We retrospectively analysed data from 324 consecutive patients treated with ECPR for OHCA at our cardiac arrest center (2018-2024). Patients without return of circulation were excluded (n=103). The remaining 221 patients were categorized based on whether Levosimendan was used during ECMO weaning and outcomes compared. The primary outcome was successful ECMO weaning, defined as survival >24 hours post-ECMO explantation. Secondary outcomes included overall survival and survival with a favorable neurological outcome, defined as a Cerebral Performance Category (CPC) score of ≥2.
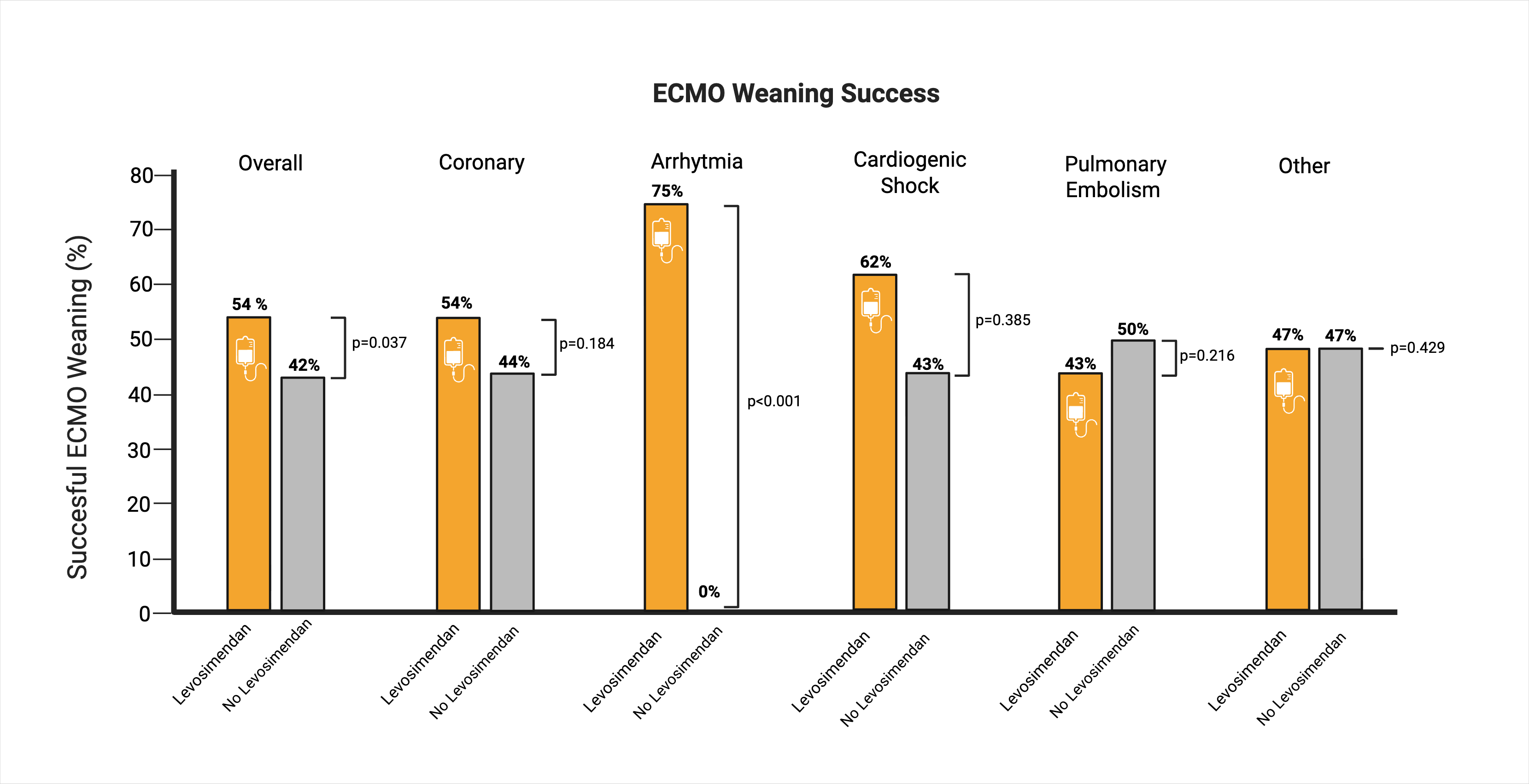
Results: Of the 221 patients included, 144 (65%) received Levosimendan during ECMO weaning. Overall, ECMO weaning was successful in 110 patients (50%). The mean ECMO run-time was 2.7 days. Patients treated with Levosimendan had a significantly higher rate of successful ECMO weaning (54% vs. 42%, p=0.037) but also displayed a longer ECMO run-time (3.1 vs. 2.1 days, p=0.007). The overall survival rate was numerically higher in the Levosimendan group (26% vs. 21%, p=0.21), with similar rates of favorable neurological survival in survivors. The prevalence of acute coronary events as the cause of cardiac arrest was significantly higher in the Levosimendan group (72% vs. 36%, p<0.0001), while pulmonary embolism rates were lower (3% vs. 13%, p=0.001). Subgroup analysis revealed that the most pronounced difference in weaning success was observed in patients with arrhythmogenic causes of arrest, where only those treated with Levosimendan were successfully weaned (75% vs. 0%, p<0.0005).
Discussion: Our results suggest that Levosimendan may positively influence ECMO weaning success. The average increase in ECMO run-time of 1 day could be attributed to the typical duration of Levosimendan administration, which averages around 24 hours. While the cause of cardiac arrest appears to affect the success of Levosimendan treatment, it is noteworthy that patients with various causes, including arrhythmogenic arrests, also benefited from this approach. Levosimendan may help mitigate post-arrest cardiomyopathy, thus facilitating ECMO weaning, regardless of the arrest cause. However, no definitive conclusions can be drawn due to the retrospective nature of this analysis and the complex, multifactorial process of ECMO weaning.
Conclusion: Levosimendan administration during ECMO weaning in ECPR patients may improve the likelihood of successful weaning and improve survival, while prolonging ECMO run-time. Further prospective studies are needed to validate these findings and explore the broader implications of Levosimendan as an adjunct in ECMO weaning protocols.