Background:
Transcatheter tricuspid valve intervention (TTVI) provides symptom relief and promotes cardiac reverse remodeling in patients with severe tricuspid regurgitation (TR). Pulmonary hypertension (PH), which frequently coexists with TR, is a known risk factor for adverse outcomes after TTVI. However, the prognostic implications of specific PH subtypes, particularly precapillary PH, and pulmonary vascular resistance (PVR) thresholds remain insufficiently defined and inconsistently reported. This study aimed to harmonize PH definitions according to current guidelines and to evaluate their association with clinical outcomes in a large, real-world TTVI cohort.
Methods:
In this international multicenter registry, 903 patients with severe TR underwent invasive right heart catheterization prior to TTVI and were followed for up to two years. PH was defined according to mean pulmonary artery pressure (mPAP ≤ or >20 mmHg). PVR was stratified per WU and according to guideline-based cutoffs. Endpoints included procedural success (device implantation with residual TR ≤ grade 2), change in NYHA functional class, and all-cause mortality.
Results:
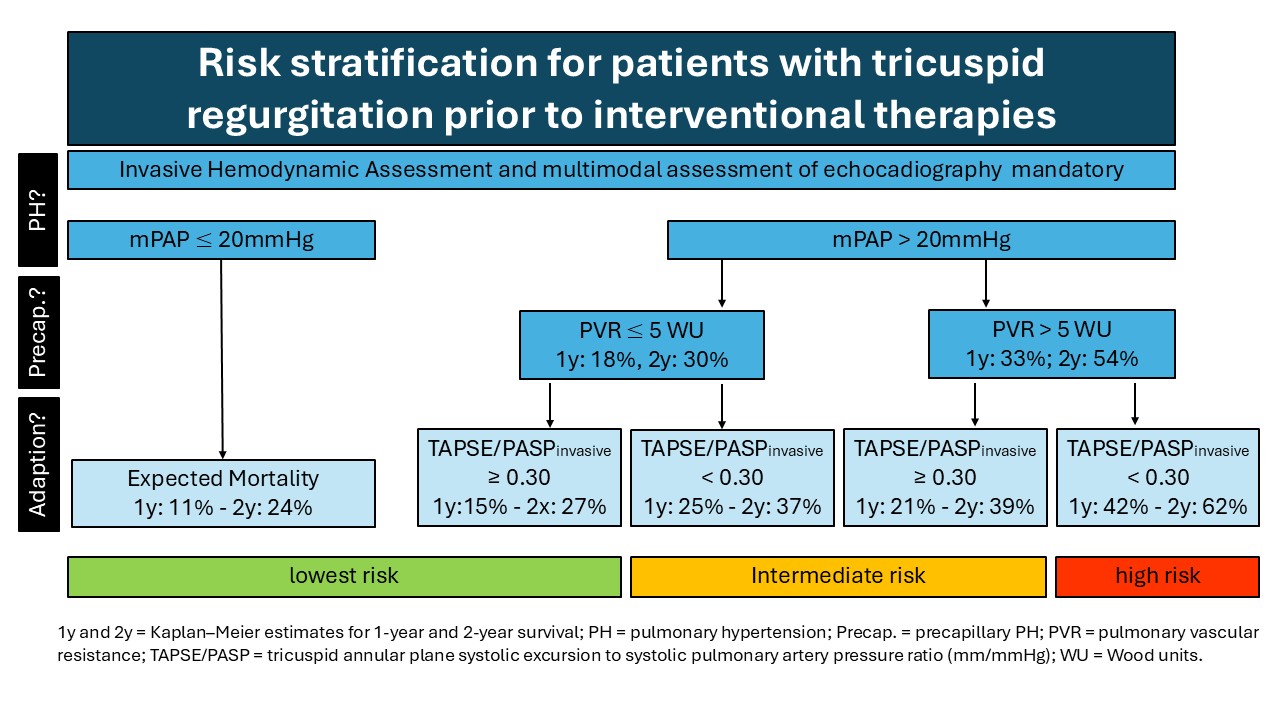
PH was present in 88% of patients, with a median PVR of 2.8 Wood units (IQR 1.9–4.0). Among patients with PH, 72% had PVR ≥2 WU and 15% had PVR ≥5 WU. The overall procedural success rate was 81%, with no significant difference across PH or PVR categories. Although patients with PH had more advanced symptoms at baseline, TTVI was associated with significant improvements in NYHA class irrespective of PH status or PVR range. One- and two-year mortality increased progressively with PH and with rising PVR, and was highest among patients with PVR ≥5 WU, the guideline-defined cut-off for severe precapillary PH. A PVR cut-off of 2 WU did not stratify patients with different survival times, as patients with PVR ≤2 WU frequently displayed a hypercirculatory phenotype, which itself is linked to adverse prognosis. However, a stepwise classification that combined PH presence, a PVR threshold of 5 WU, and the TAPSE/PASP ratio (<0.30 vs. ≥0.30 mmHg/mm) allowed refined risk stratification (see figure).
Conclusion:
In this large real-world cohort, severe precapillary PH was relatively uncommon and typically less pronounced than in pulmonary arterial hypertension populations. TTVI achieved high procedural success and symptomatic improvement across all PH and PVR subgroups. However, mortality increased with higher PVR, particularly beyond 5 WU. Incorporating hemodynamic profiling, including PH presence, PVR burden, and right ventricular adaptation, enhances pre-procedural risk assessment and patient selection for TTVI.