Background: Immune checkpoint inhibitors (ICI) are gaining relevance for an increasingly broad spectrum of cancers, acting by modulating the bodily immune system to fight tumor cells. This mechanism of action comes with the possibility of several autoimmune adverse effects, including ICI-associated myocarditis. In this developing field, our aim was to analyze the incidence, severity and prognosis of ICI-associated myocarditis in melanoma patients, treated with at least one ICI.
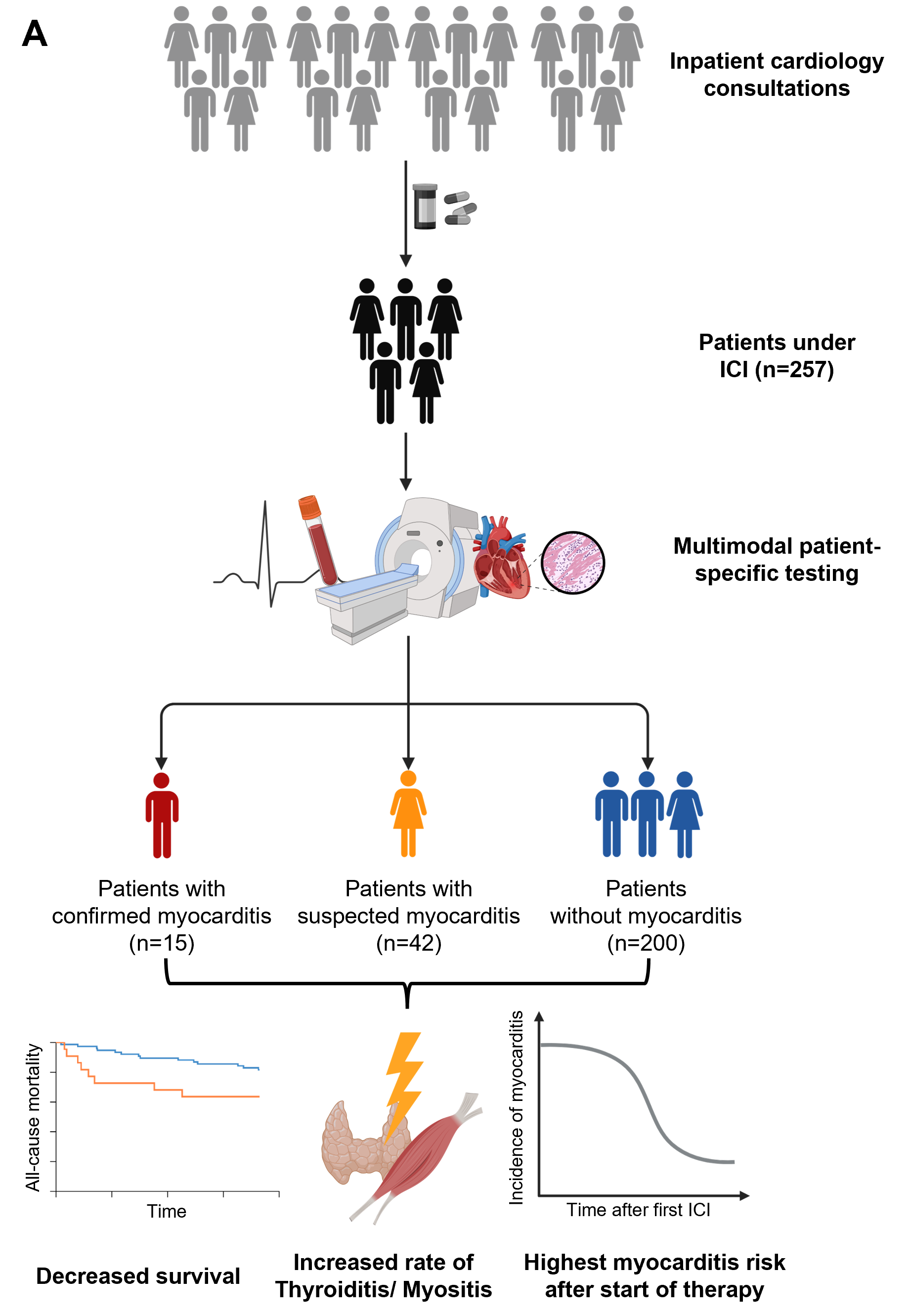
Methods and results: This is a retrospective, single-centre, observational study. We enrolled 257 patients, who were treated with ICI between 2018 and 2024 at the University Hospital of Tübingen, Germany. All patients were assessed by cardiologists at our department before therapy initiation and/or for various heart complaints. Patients were followed-up for at least 360, up to a maximum of 1440 days after initiation of ICI therapy. In 200 out of 257 (78%) patients, no signs of myocarditis could be detected. The remaining 57 (22%) patients were further grouped into those with “suspected myocarditis” or “confirmed myocarditis”. Suspected myocarditis was diagnosed in 42 patients (16%), based on clinical findings including dyspnoea and chest pain. Confirmed myocarditis, containing 15 out of 257 patients (6%) was defined by a pathologic cardiac MRI or biopsy and elevated cardiac biomarkers. The highest incidence of suspected and confirmed myocarditis was found in the first 360 days of the follow-up period. 12 out of 15 (80%) confirmed cases occurred up until 5 months after the first ICI treatment dose. Comparison of the ICI-treated control and the myocarditis group revealed a trend towards decreased survival in the latter group in a one-year follow-up (p=0.07). Kaplan-Meier estimates showed the steepest decrease in survival in the first days after diagnosis, with a realignment of the curves in the later period of follow-up. Among the 7 administered drugs, Cemipilimab showed a higher incidence of myocarditis (20%) when compared to other drugs (6%). Furthermore, a significant coincidence of myocarditis with myositis and thyroiditis (p<0.05), but not with other ICI-associated side effects, was observed.
Conclusion: These data show real-word, preselected patients, treated for melanoma at a German university hospital. In this preselected group, a considerable number of patients showed symptoms suggestive for myocarditis. Myocarditis was confirmed in only a fraction of the patients. However, patients with both suspected and confirmed myocarditis showed increased mortality when compared to those without signs of myocarditis. Incidence of myocarditis was higher after therapy initiation and myositis as well as thyroiditis were side effects commonly seen in combination with myocarditis.