AIMS: Given the growing recognition of right heart failure and tricuspid regurgitation as a determinant of outcome, treatment strategies have rapidly evolved, including the advent of transcatheter tricuspid valve replacements (TTVR) systems. Recent data showed the importance on outcomes and procedural success in patients undergoing tricuspid edge-to-edge repair, a connection, not yet explored in patients undergoing TTVR. We therefore aimed to investigate whether invasive hemodynamic assessment of biventricular congestion is associated with two-year mortality after TTVR.
METHODS: Patients undergoing orthotopic TTVR between 2019 and 2025 at two high-volume centers were included. All patients underwent preinterventional right heart catheterization to quantify filling pressures and to assess pulmonary hypertension. The associations of mean right atrial pressure (RAP) and pulmonary capillary wedge pressure (PCWP) with two-year all-cause mortality were analyzed after stratification by the respective median values.
RESULTS: A total of 80 patients (median age 78 years [IQR 73 – 84], 70% female) were included. All implanted TTVR device types (82% Evoque, 14% LuxValve and 4% others) achieved a significant procedural reduction of tricuspid regurgitation (preprocedural TR grade 5 (IQR 4 – 5) vs. postprocedural TR grade 1 (IQR 0 – 1), p<0.001).
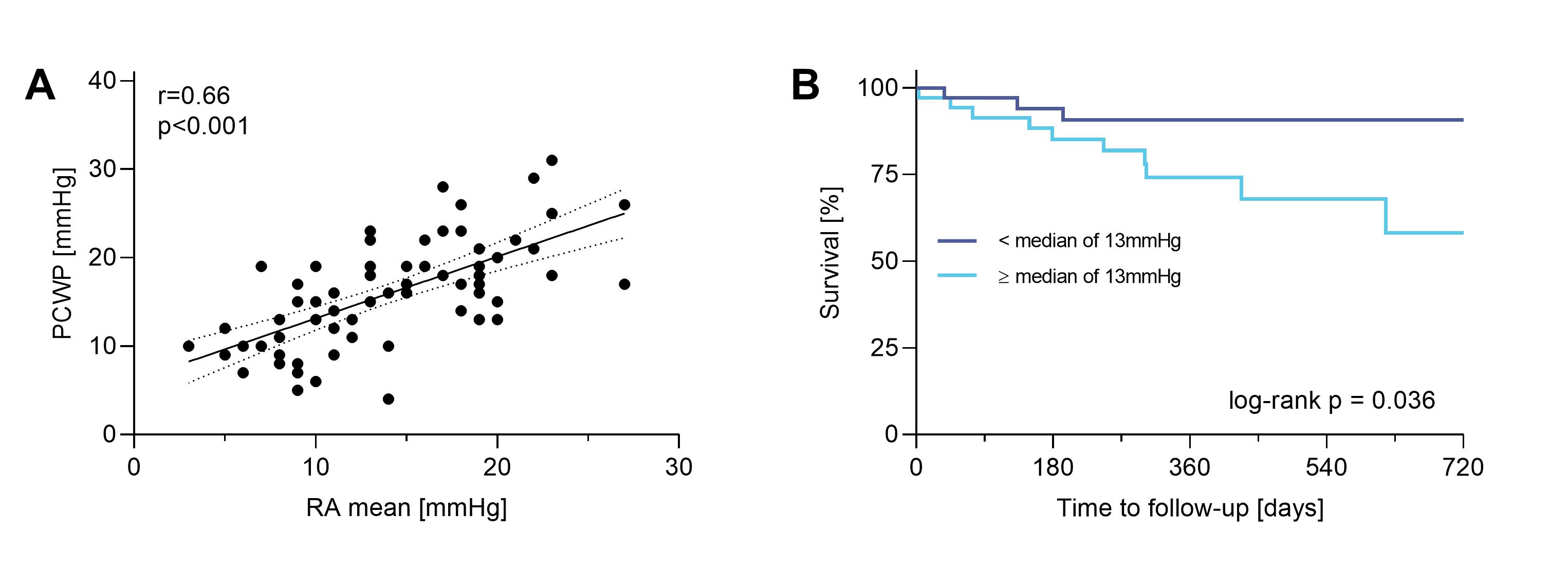
Preinterventional hemodynamic assessment revealed elevated median RAP (13 mmHg [IQR 13-18]), mild pulmonary hypertension (mean pulmonary artery pressure 24 mmHg [IQR 19 – 28]), and elevation of PCWP (16 mmHg [IQR 12 – 19]). Mean RAP and PCWP showed a strong linear correlation (r=0.66; R² = 0.44; p<0.001, Fig 1A). Within a median follow-up of 416 days (IQR 220-720) 15 (20 %) patients died. While PCWP was not associated with survival (log-rank p=0.77), Kaplan-Meier analysis identified a significant association between elevated RAP and two-year all-cause mortality (log-rank p=0.036, Fig 1B). Notably, on multivariable analysis this was independent of baseline TR severity (HRadj 4.57, 95% CI 1.22 to 17.15).
CONCLUSION: Beyond tricuspid valve pathology itself, this study highlights biventricular congestion as a key hemodynamic feature in patients with isolated significant tricuspid regurgitation. Despite a strong correlation between right- and left-sided filling pressures, only elevated RAP was associated with increased two-year mortality, even after procedural success with reduction of tricuspid regurgitation to a minimum. These findings emphasize the relevance of preinterventional hemodynamic evaluation and raise the hypothesis that intensified pre-interventional decongestion might favorably impact survival warranting confirmation in dedicated future studies.
Figure 1: