Objective:
This study introduces a novel method for quantifying aortic valve calcification (AVC) using contrast-enhanced computed tomography (CECT) data. Standard quantification of AVC is typically performed using non-contrast-enhanced CT (NCCT), expressed as the Agatston score (AGS). Previous attempts to assess AVC using CECT have been hindered by methodological challenges, including potential over- or underestimation due to fluctuations in blood density within the ascending aorta and variations in contrast agent concentration.
Methods:
To overcome these limitations, this study proposes a novel, contrast-adjusted approach for AVC quantification which is evaluated retrospectively on a novel, single-center dataset of N=234 patients (56.8% females, age: 80.9 ± 6.6 years) with suspected severe aortic valve stenosis who underwent NCCT and CECT. A log-linear regression model for AVC quantification for individual patients at specific contrast agent concentrations was developed. For population-level assessment, a multivariate regression model was employed, and validated through repeated random subsampling in different 70%/30% train/test splits.
Results:
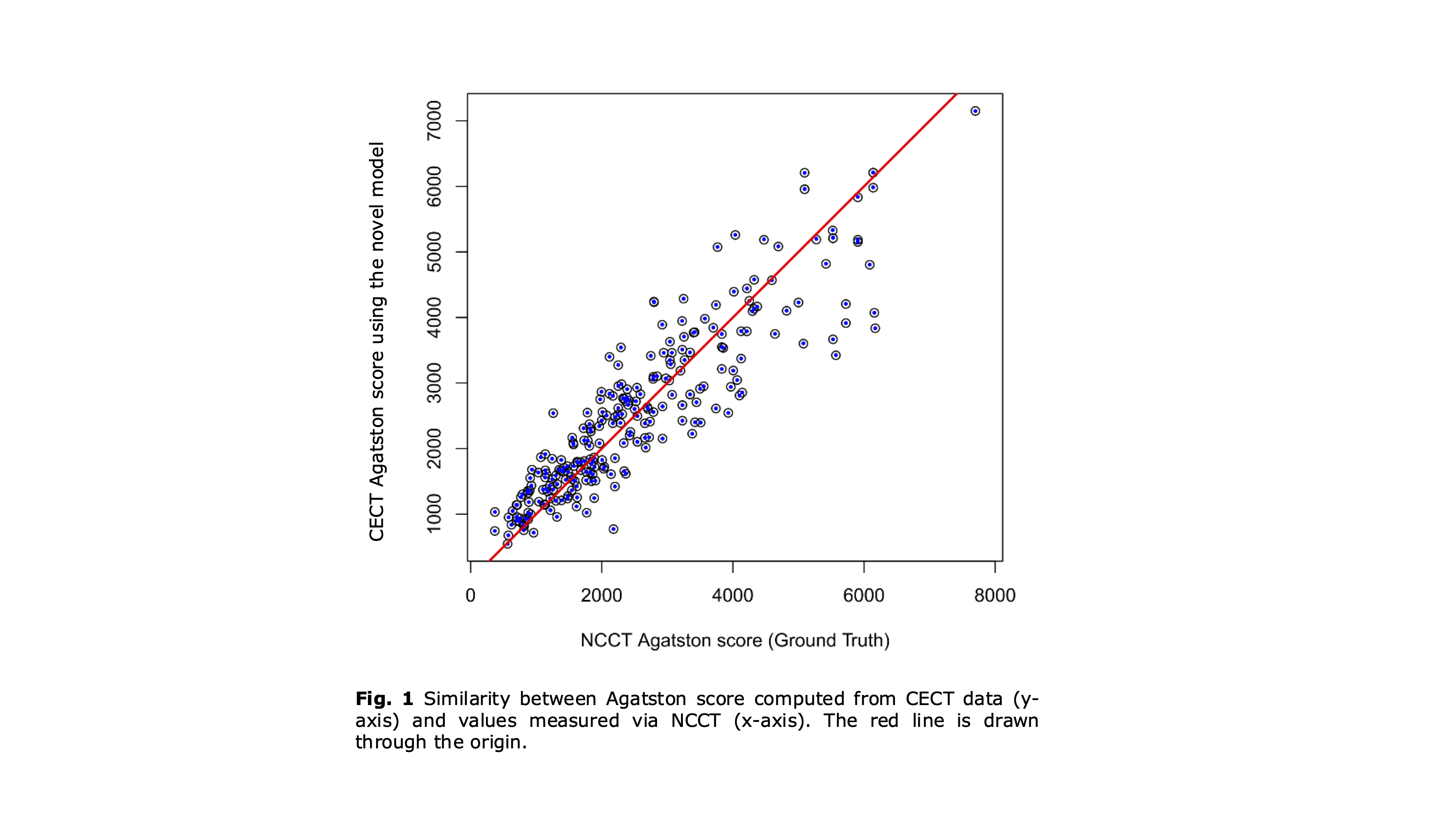
Results outperform state-of-the-art methods by reaching an adjusted R2 value of 0.95. Robust performance in relevant subgroups; e.g. in patients with low flow, low-gradient aortic stenosis are observed with residuals not differing from the rest of the cohort. Moreover, in patients at diagnostically critical range with AGS ≤ 2000, residuals were smaller in median and interquartile range compared to higher AGS patients.
Conclusions:
Our results demonstrate the potential of assessing AVC using CECT alone in a single center study and highlight the added value of contrast adjustment.