Background: The clinical context and coronary disease complexity may influence the diagnostic performance of physiological assessment tools. While Quantitative Flow Ratio (QFR) provides a non-invasive, angiography-based evaluation of lesion significance, its predictive accuracy in multivessel disease, acute coronary syndromes (ACS), and in vessels that have undergone percutaneous coronary intervention (PCI) has not been sufficiently investigated.
Methods: Patients who underwent cardiac Magnetic Resonance Imaging (MRI) between January 1 and December 31, 2024 were included. MRI was performed to further evaluate residual or intermediate lesions identified during angiography. QFR analysis was retrospectively conducted using Medis QFR® 3.0 (Medis Medical Imaging Systems, Leiden, The Netherlands). The correlation between QFR and MRI-detected ischemia was analyzed across subgroups according to clinical presentation (ACS vs. elective), revascularization status (PCI vs. conservative approach), and disease extent (single- vs. multivessel) (Figure 1).
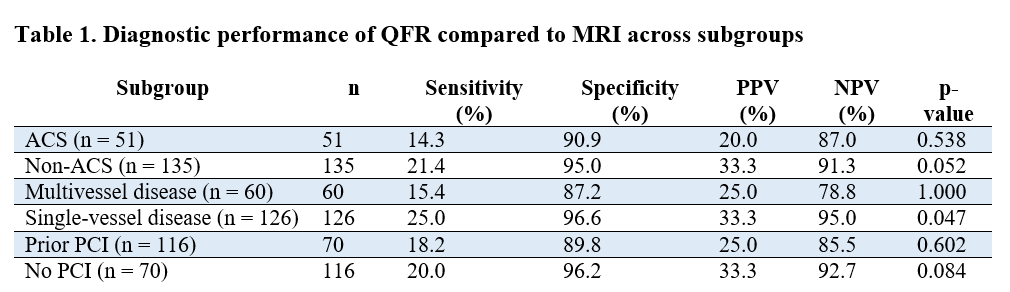
Results: Coronary angiographies of 186 patients were analyzed across different clinical and procedural settings. Diagnostic performance of QFR varied substantially depending on presentation, disease complexity, and preceding intervention. In ACS, the agreement between QFR and MRI was low (p = 0.54), whereas in non-ACS cases higher specificity and predictive accuracy were observed (p = 0.052). Similarly, QFR demonstrated less reliable results in multivessel disease (p = 1.00) and following PCI (p = 0.602), while performance was better in single-vessel (p = 0.047) and no-PCI settings (p = 0.084), reflected by higher specificity and negative predictive values. These differences likely reflect the influence of lesion complexity, microvascular dysfunction, and post-procedural hemodynamic changes on QFR estimation (Table 1).
Conclusions: QFR showed variable diagnostic performance across clinical and procedural settings. Its agreement with MRI was strongest in stable, single-vessel disease without prior intervention, while accuracy decreased in ACS, multivessel, and post-PCI conditions.