BackgroundValidated approach for the detection of disease progression (DiP) in transthyretin amyloid cardiomyopathy (ATTR-CM) exists, yet predicting DiP under disease-modifying therapy remains an unmet clinical need.
ObjectivesTo identify parameters with discriminative ability for predicting DiP and to develop a risk stratification model for DiP in ATTR-CM patients receiving disease-modifying therapy.
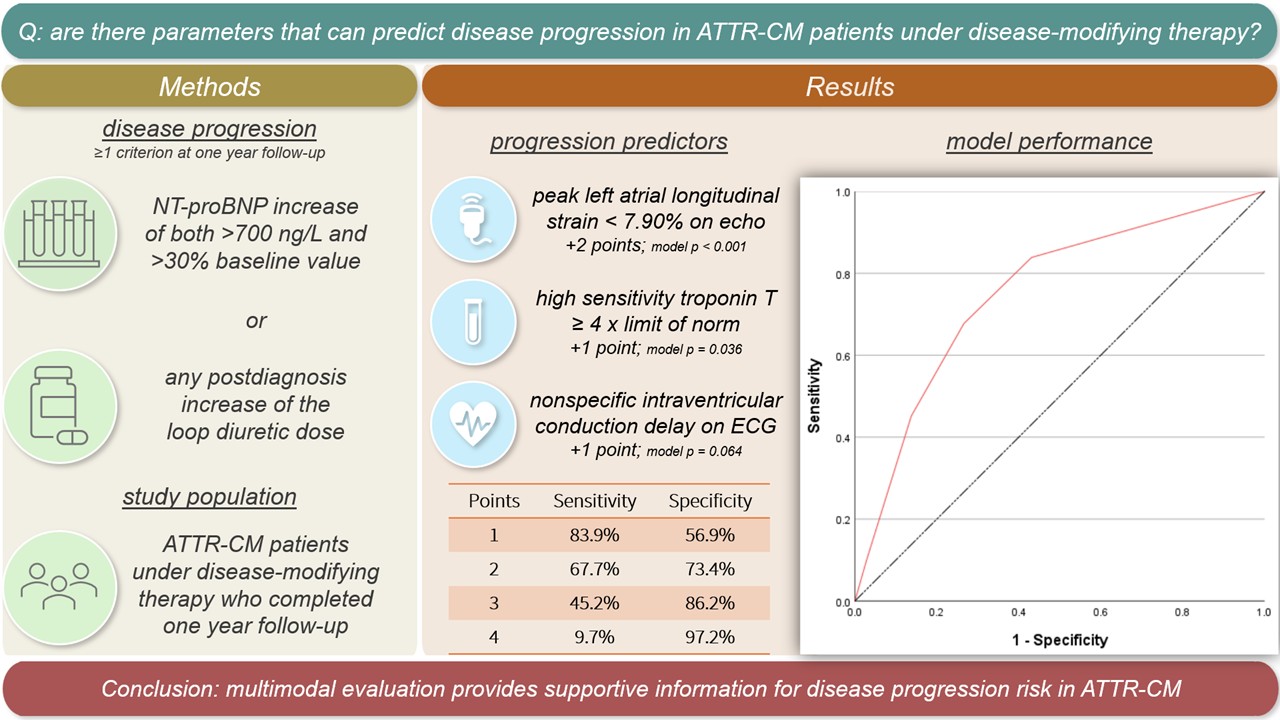
MethodsIn this prospective registry study, we included all ATTR-CM patients who received disease-modifying therapy and completed one-year follow-up at the Amyloidosis Center Charité Berlin. DiP was defined according to validated criteria involving sufficient NT-proBNP rise or any loop diuretic dose increase at one-year follow-up (Ioannou, A, Cappelli, F, Emdin, M. et al. Stratifying Disease Progression in Patients With Cardiac ATTR Amyloidosis. JACC. 2024 Apr, 83 (14) 1276–1291.). Except for DiP and follow-up-related parameters, all data were obtained exclusively from examinations performed as part of the initial diagnostic assessment. Left atrial strain measurements were performed in line with current guidelines, using 2D speckle tracking echocardiography, measured according to the zero strain reference at end-diastole.
Results
Among 171 included patients, 62 (36%) met criteria for DiP. General characteristics at baseline visit were largely comparable between groups; however, progressors exhibited greater dyspnea burden and nearly 2.5-fold higher prevalence of nonspecific intraventricular conduction delay (NICD) on ECG. Median high-sensitivity troponin T levels were 70% higher among progressors (34 vs. 58 ng/L, p < 0.001). Moderate tricuspid regurgitation was the only conventional echocardiographic parameter significantly associated with DiP, occurring approximately twice as frequently among progressors. Left atrial function analysis identified peak left atrial longitudinal strain (PALS) < 7.90% as the most discriminative among all evaluated parameters (Youden’s index 38.8%). A multivariable risk model integrating NICD, high-sensitivity troponin T, and PALS achieved an AUC of 0.75 (95%CI: 0.68-0.83) for predicting DiP.
Conclusion
Multimodal evaluation provides prognostic information regarding DiP risk in ATTR-CM patients undergoing disease-modifying therapy. Findings of this study may support clinical decision-making and improve identification of high-risk patients, who may benefit from intensified monitoring.