Background:
Severe tricuspid regurgitation (TR) is associated with poor outcomes and affects a growing proportion of elderly patients. Emerging transcatheter approaches, such as tricuspid transcatheter edge-to-edge repair (T-TEER) and annuloplasty (TTVA), rely heavily on three-dimensional echocardiography for procedural guidance. While 3D vena contracta area (3D-VCA) has shown superior accuracy over conventional two-dimensional parameters in assessing TR severity, its predictive value and definitive cut-offs for transcatheter interventions remain unclear.
Methods:
This is the first retrospective analysis of residual 3D VCA in high-surgical-risk patients who underwent T-TEER or TTVA at a tertiary center in Germany (n=141). Echocardiographic data were acquired using standardized 2D transthoracic and 3D transesophageal protocols with offline analysis. The primary endpoint was 3-year survival.
Results:
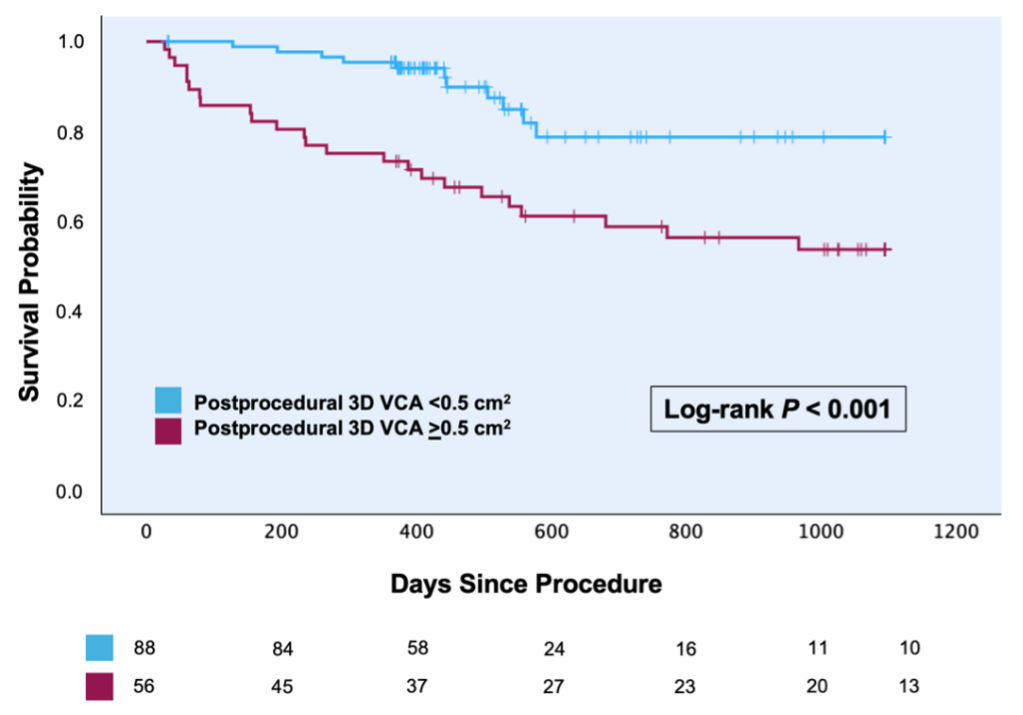
The study cohort were predominantly women (68.3%), with a median age of 81 years (76–84). The median TRI-Score was 4 (3–6). Residual TR grade ≤II was achieved in 69% of procedures. Over a median follow-up period of 473 (375–891) days, univariate cox regression showed a significant association of 3D VCA and survival (HR 1.16 [1.02 – 1.33]; p=0.029). Via maximally selected rank statistics a cut-off value of >0.5 cm2 was determined. Patients with a postprocedural 3D VCA above this value showed significantly poorer survival (p<0.001). Different proposed cut-off-values for severe TR by several authors also showed significant differences in survival in this cohort (p=0.004 for 3D VCA >0.4 cm2 and >0.61 cm2, p<0.001 for >0.75 cm2). Conventional parameters effective regurgitation orifice area (EROA) ≥ 0.4 cm² and VC ≥ 7 mm showed no significant association with survival (log-rank test: p=0.46 and p=0.07, respectively). A 3D VCA cut-off of 0.2 cm2, differentiating mild from moderate TR, did not yield significant influence on 3-year survival (p=0.16).
Multivariate cox-regression analysis incorporating postprocedural 3D VCA (categorial cut-off 0.5 cm2, baseline NYHA level (I-IV), and TRI-SCORE (points), showed a significant association of 3D VCA and TRI-SCORE with survival with no such association for NYHA level (p=0.012, <0.001, and 0.34, respectively).
Conclusion:
In this study, postprocedural 3D VCA was independently associated with 3-year survival, and postprocedural 3D VCA >0.5 cm2 served as a meaningful cut-off value. In contrast, the conventional cut-off values for EROA and VC showed no significant associations with survival. Our findings reinforce the importance of maximizing procedural efficacy to improve patient outcomes and demonstrate a potential predictive value of 3D VCA assessment.