Background: The assessment of intermediate coronary lesions poses significant challenges in clinical practice. Angiography and quantitative coronary analysis offer anatomical insights, while intravascular imaging refines the evaluation of plaque and vessel morphology; however, determining the physiological impact of a lesion still relies on invasive pressure-wire assessment. Quantitative Flow Ratio (QFR) offers a non-invasive alternative that may bridge the gap between anatomical and functional evaluation. While validation studies have focused on fractional flow reserve, the correlation between QFR and cardiac Magnetic Resonance Imaging (MRI) has not yet been investigated.
Methods: Patients who underwent MRI between January 1 and December 31, 2024 for additional assessment of intermediate coronary lesions were included. A total of 186 cases with available angiographies were identified, and QFR analysis was retrospectively performed using Medis QFR® 3.0 (Medis Medical Imaging Systems, Leiden, The Netherlands). The aim was to evaluate the correlation between QFR- and MRI-detected ischemia (Figure 1).
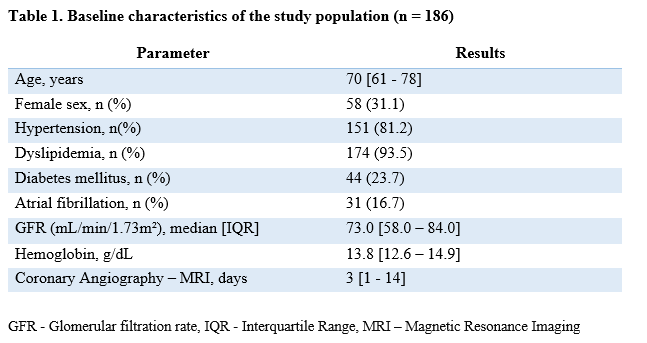
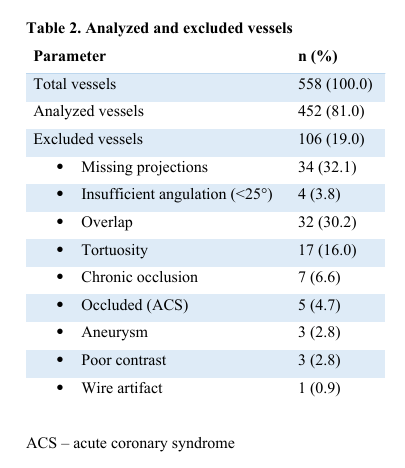
Results: Overall, 452 vessels in 186 patients were analyzed. The median interval between coronary angiography and MRI was 3 days [1 - 14]. The baseline characteristics of the study population are presented in Table 1. A total of 106 vessels (19.0%) were excluded due to missing projections, insufficient angulation, overlap, tortuosity, wire artifact, aneurysm, or chronic occlusion (Table 2). The median QFR value was 0.92 [0.89–0.95] for the left anterior descending artery (LAD), 0.98 [0.95–0.99] for the left circumflex artery (LCX), and 0.95 [0.92–0.98] for the right coronary artery (RCA). Pathological findings on cardiac MRI indicating regional myocardial ischemia were present in 21 cases (11.3%), whereas pathological QFR values (≤0.80) were observed in 17 vessels (9.1%) across 14 patients (7.5%). Paired analysis of QFR and MRI yielded a negative predictive value of 90.1% and a positive predictive value of 28.6%.
Conclusion: QFR represents a promising tool for the non-invasive physiological assessment of coronary lesions. However, its validity remains limited by technical and anatomical factors such as vessel tortuosity, overlap, aneurysms, and suboptimal angiographic projections. Despite these constraints, QFR demonstrated a high negative predictive value and may therefore can be used as a reliable method to exclude functionally significant stenoses during coronary angiography.