Background: Current ESC-guidelines on the management of patients after acute myocardial infarction (AMI) only include the assessment of left ventricular function by left ventricular ejection fraction (LVEF) in addition to clinical risk scores to estimate prognosis. However, patients may face an unfavourable prognosis after AMI despite a normal or only moderately reduced LVEF. Existing data suggests that various echocardiographic parameters could be useful for risk stratification after AMI, including mitral regurgitation (MR), left atrial volume index (LAVI) or LA reservoir strain. However, these data are often contradictory regarding the different parameters.
Aim: We aimed to evaluate the incremental association of MR, LA reservoir strain and LAVI in our large all-comers cohort, postulating that severe MR in patients after AMI is associated with a reduced survival rate, with reduced LA reservoir strain and elevated LAVI posing an additional risk.
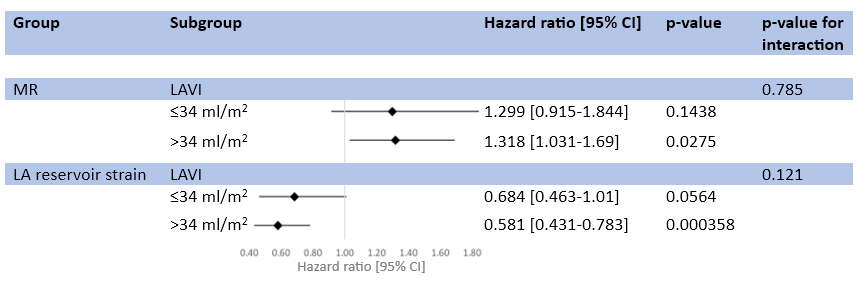
Methods: This analysis is based on the ECAD registry of patients undergoing conventional coronary angiography at the Department of Cardiology and Vascular Medicine at the University Clinic Essen between 2004 and 2019. For the present analysis we included patients with AMI, who had available echocardiographic and survival information. Cox regression analysis, adjusting for age, sex, systolic blood pressure, low-density lipoprotein (LDL) cholesterol, smoking status, diabetes, and family history of premature coronary artery disease. Effect sizes were depicted per 1 standard deviation increase in LAVI or LA reservoir strain or presence of at least moderate MR. In addition, subgroup analysis was performed, stratifying by LAVI ≤ and > 34 ml/m2.
Results: 1621 patients (74.5% male, mean age 65 years) were included. We observed a significant correlation between MR and LAVI (r=0.43, p<0.0001), MR and LA reservoir strain (r=-0.40, p<0.0001), and LAVI and LA reservoir strain (r=-0.41, p<0.01). Patients that died within a median of 1.5 (0.5; 4.1) years of follow-up had a larger LAVI (37.0 (29.6; 48.1) ml/m2 vs. 32.6 (26; 41.4) ml/m2, p<0.001), more often at least moderate MR (33.7% vs. 20.1%, p<0.001) and a lower LA reservoir strain (15.4±7.96% vs. 21.1±9.14%, p<0.001). In multivariable cox regression analysis, at least moderate MR (1.289 [1.077-1.543], p=0.0056), LAVI (1.247 [1.053-1.477], p=0.011) and LA reservoir strain (0.577 [0.460-0.724], p<0.001) were significantly associated with mortality. After dividing the cohort into patients with a LAVI ≤ vs. >34 ml/m2, MR and LA reservoir strain remained independently associated with mortality (Figure 1). In receiver operating characteristics, combination of MR, LAVI, and LA reservoir strain improved the prediction of mortality above traditional risk factors (AUC 0.727 to 0.775, p=0.049).
Conclusion: In the present large registry of patients presenting with AMI, at least moderate MR, LAVI and LA reservoir strain incrementally and independently predicted long-term mortality. Our results indicate that despite a strong correlation, MR, LAVI and LA reservoir strain, a comprehensive assessment provides the most accurate prediction of prognosis for AMI patients.