Background: Mitral transcatheter edge-to-edge repair (M-TEER) has emerged as a standard procedure for treatment of severe mitral regurgitation (MR). However, patient and device selection, procedural success and outcomes have changed over time. Therefore, we aimed to analyse the temporal development of M-TEER focusing on MR aetiologies, patient comorbidities, procedural success and outcomes.
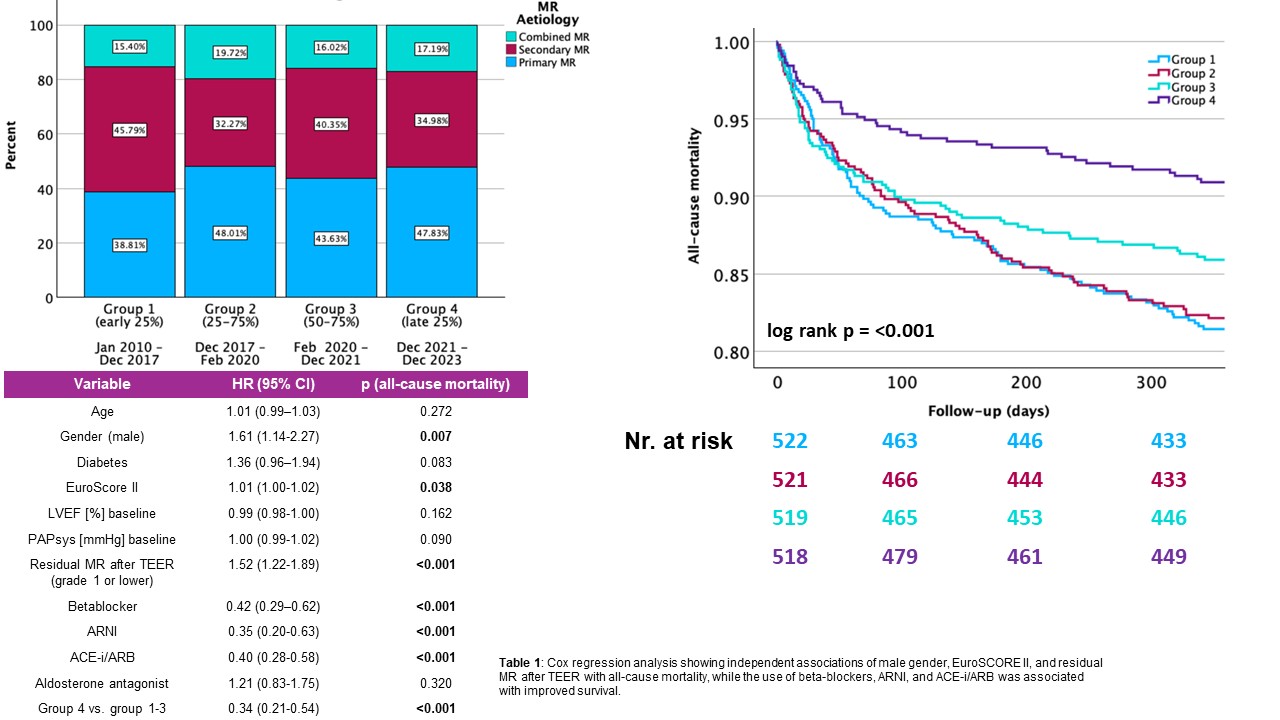
Methods and results: This is a retrospective, multicentre, study. We enrolled 2,080 patients, who were treated with the Abbott MitraClip™ and the Edwards PASCAL™ systems between 2010 and 2023 at two German heart centers in Baden-Württemberg. Patients were split into four quartiles to create similar sample size. 522 patients received the device between 2010 and 2017 (group 1), 521 patients between 2017 and 2020 (group 2), 519 patients between 2020 and 2021 (group 3) and 518 patients between 2021 and 2023 (group 4). The proportion of treated primary MR increased (from 38.81% to 47.83%), whereas secondary MR decreased (from 45.79% to 34.98%). Rates of mixed aetiology remained constant (from 15.50 to 17.19%).
Kaplan-Meier analysis revealed significant differences in 1-year all-cause mortality across the four groups (log-rank p<0.001), with group 4 (2021-2023) showing significantly improved survival compared to earlier cohorts.
Multivariable Cox regression analysis identified following variables as independent predictors of mortality: residual MR >1 (HR 1.52, p<0.001), male gender (HR 1.61, p=0.007), EuroSCORE II (HR 1.01, p<0.038) and the prescription of betablockers (HR 0.42, p<0.001), ARNIs (HR 0.35, P<0.001) and ACE-is/ARBs (HR 0.40, p<0.001). Further, group 4 showed significantly decreased mortality when compared to groups 1-3 (HR 0.34, p<0.001). Age, diabetes, left ventricular ejection fraction, baseline pulmonary artery pressure and treatment with aldosterone antagonists did not show independent associations with the respective outcome.
Conclusion: One-year survival after M-TEER improved significantly over time, paralleled by shifts in MR aetiology. These findings likely reflect advances in procedural expertise, optimized patient selection, and improved peri-interventional and heart failure management. Continuous refinement of these aspects may further enhance outcomes in this high-risk patient population.