Background
Women with atrial fibrillation (AF) demonstrate a higher prevalence of low-voltage areas (LVA) compared with men. However, the prognostic significance of LVA in women remains unclear. Previous studies suggest that female patients may require a greater substrate burden for LVA to predict recurrence and could benefit from tailored ablation approaches. Evidence from trials on pulmonary vein isolation with adjunctive substrate modification remains mixed, and sex-specific data, particularly in paroxysmal AF are limited.
Methods
We analyzed 363 women (median age 73.6 years) undergoing first pulmonary vein isolation (PVI) using an ablation-index-guided, high-power short-duration (HPSD) CLOSE protocol at Deutsches Herzzentrum der Charité (2019–2024). High-resolution 3D voltage mapping was performed prior to ablation. LVA were defined as bipolar voltage <0.5 mV. The primary endpoint was arrhythmia recurrence (>30 s AF, atrial flutter or atrial tachycardia) after a 3-month blanking period.
Results
LVA were present in 36.9% of women, predominantly in septal (33.8%) and posterior (12.9%) regions. Over a median follow-up of 14.0 months, recurrence occurred in 39.7%. In paroxysmal AF, recurrence rates were significantly higher in women with LVA versus without LVA (51.9% vs. 27.0%, p<0.001). In persistent AF, recurrence did not differ by LVA status. Kaplan-Meier curves are shown in figure 1. In multivariate Cox regression, persistent AF remained an independent predictor of recurrence (HR 0.43, 95% CI 0.26–0.69), whereas LVA showed a strong effect size without reaching significance.
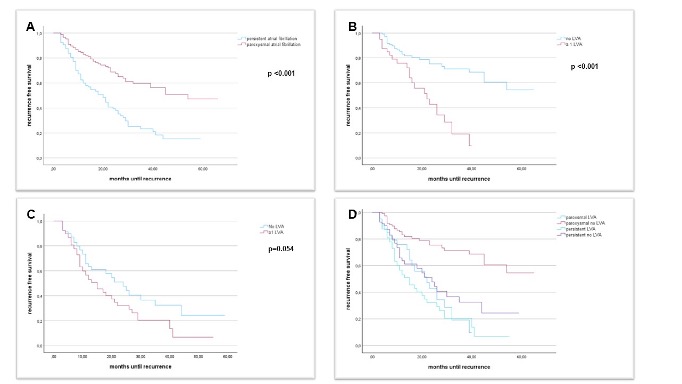
Figure1:
Kaplan–Meier curves showing recurrence-free survival in patients with A: paroxysmal vs. persistent atrial fibrillation; B: paroxysmal atrial fibrillation and LVA vs. no LVA; C: persistent atrial fibrillation and LVA vs. no LVA; D: persistent and paroxysmal atrial fibrillation, LVA and no LVA; LVA: Low voltage areaConclusion
In women undergoing first PVI, LVA were common and associated with higher recurrence in paroxysmal, but not persistent AF. These findings suggest that LVA may have different prognostic implications in female patients with paroxysmal AF and support consideration of sex-specific ablation strategies. Notably, all previous randomized trials evaluating adjunctive substrate modification beyond PVI included only patients with persistent AF, leaving the potential benefit of a PVI-plus approach in women with paroxysmal AF and LVA unexplored. This question gains importance in the era of increasing single-shot PVI adoption, which may limit tailored substrate treatment.



