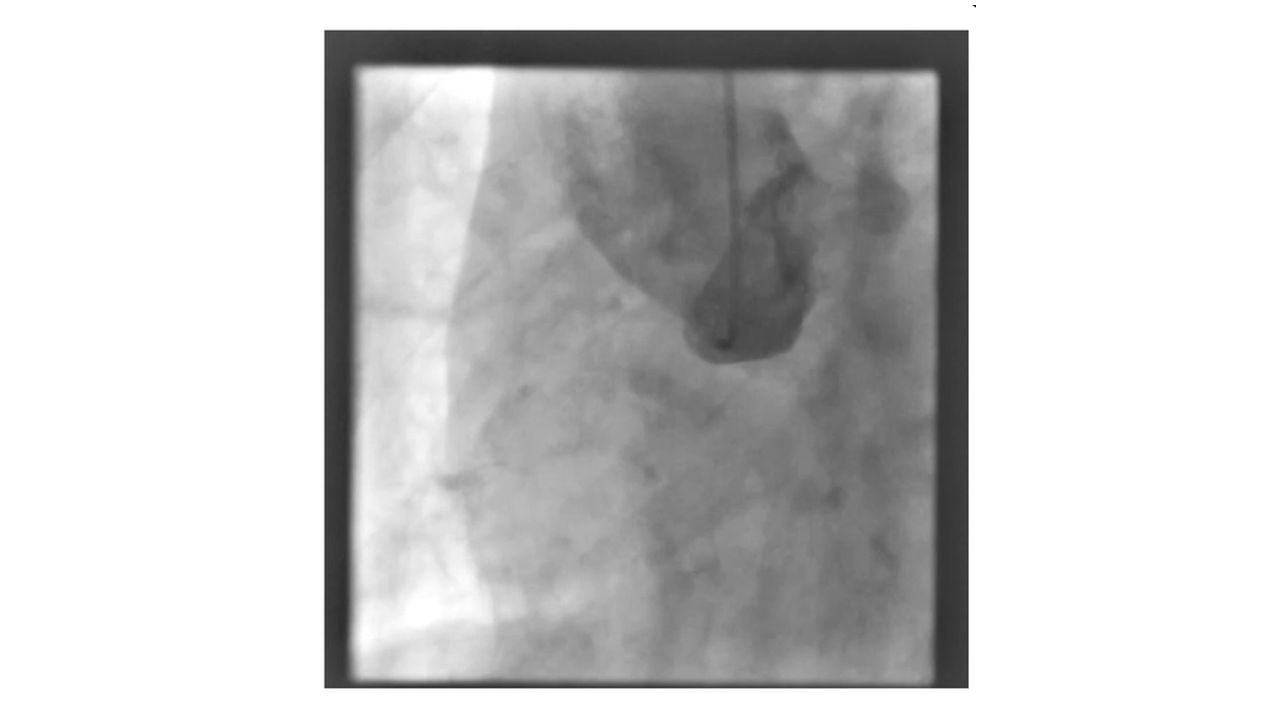
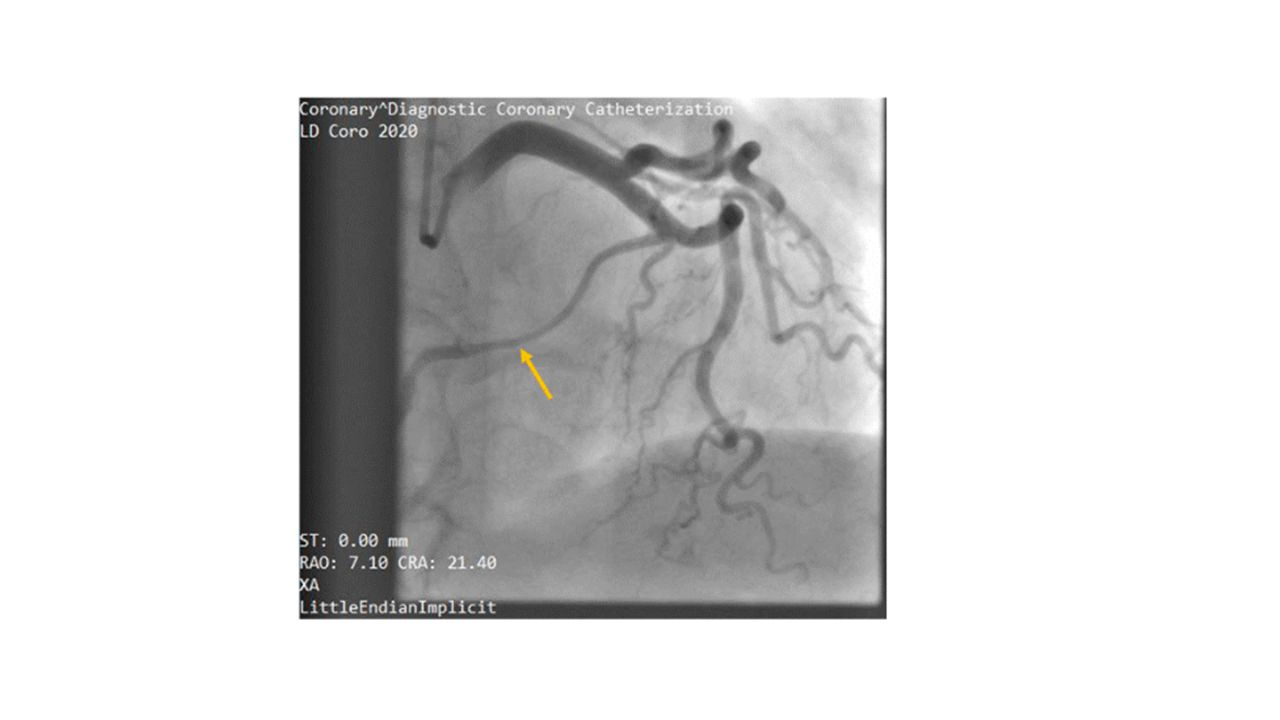
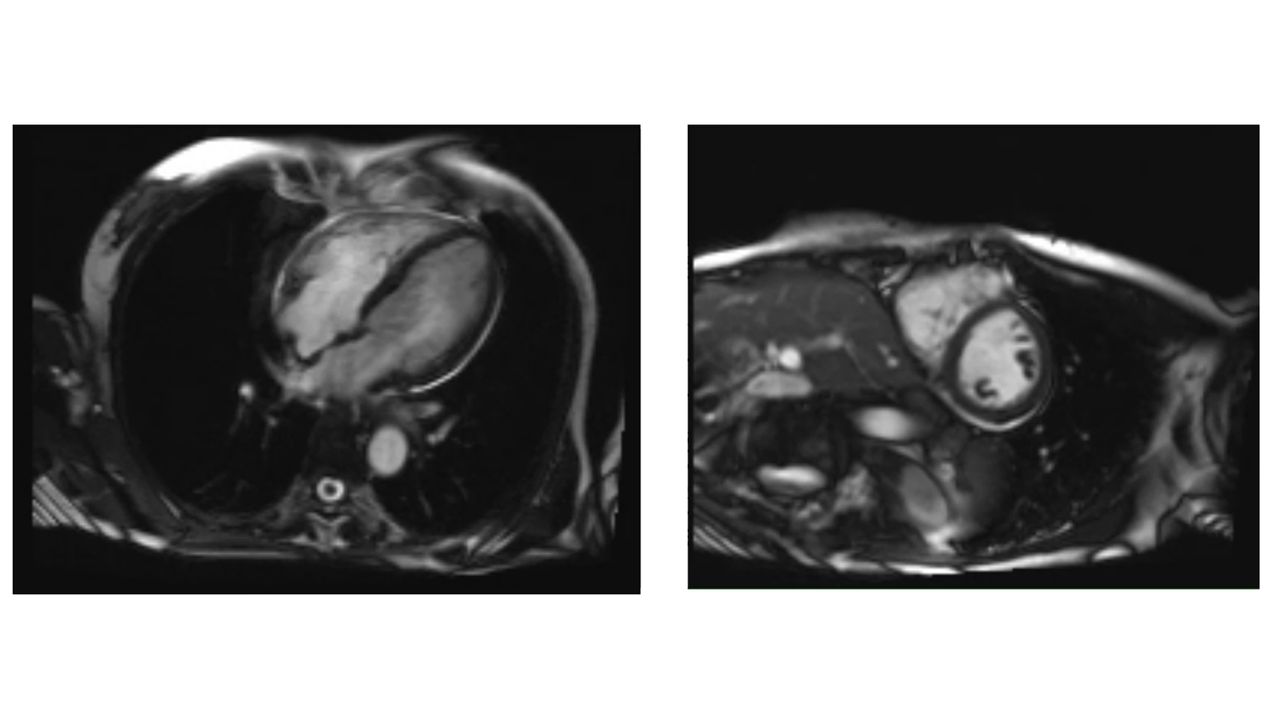
A 68-year-old woman presented for elective coronary angiography after 4 months of angina pectoris, described as compressing or stitching chest pain without radiation, occurring intermittently at rest and on exertion. Previous cardiology evaluation with resting ECG and echocardiography was normal. She was a heavy smoker for over 25 years and had dyslipidemia and a double left kidney. Labs: eGFR 95 ml/min, LDL 73 mg/dl, HbA1C 6%. Resting ECG: sinus rhythm, 95 bpm, normal axis, no significant ST-T changes. Echocardiography: normal LV systolic function, no wall motion or valvular abnormalities. Coronary angiography revealed angiographically normal left coronary artery with suspected retrograde flow to the RCA. Despite multiple attempts with various catheters and views, RCA cannulation was unsuccessful. We performed aortic root angiography using a 5 Fr. pigtail diagnostic catheter which failed to depict the RCA. The first differential diagnosis was an ostial RCA-chronic total occlusion (CTO) with retrograde filling from a large septal branch from LAD, and we decided to plan for elective PCI and recanalization of the RCA-CTO. A meticulous evaluation of the angiographic views by our CTO-/CHIP-team during planning for PCI revealed that the RCA flow seems to be an antegrade rather than retrograde flow, contrary to the initial assumption. Tracing the course of the large second septal branch demonstrated that, it follows the anatomical course of RCA. We performed a computer tomography angiography (CTA) to confirm the diagnosis and exclude malignant course of the suspected anomalous RCA. Additionally, an abdominal CT was performed to evaluate the abdominal organs for any associated congenital anomalies. CTA confirmed the diagnosis, demonstrating that RCA was originating anomalously from the mid-segment of LAD. The anomalous RCA runs firstly between the two great arteries (aorta and pulmonary arteries), then antero-lateral in the groove between the right atrium and right ventricle and curved posteriorly to reach the postero-inferior wall between the left and right ventricles. CT abdomen showed a double left kidney with double ureters; other abdominal organs were normal. Stress imaging was done to assess stress-induced ischemia and cardiovascular risk. Cardiac MRI showed no ischemia, normal LV morphology and function, and no wall motion abnormalities. No late gadolinium enhancement indicating ischemia or prior myocarditis was found. Conservative treatment and a risk factor control were chosen. To our knowledge, this is the first reported case of a malignant inter-arterial course anomalous RCA from the mid-LAD.
Learning objectives
-In case of suspected coronary anomalies or unclear coronary course and/or origin a CTA is strongly recommended
-Do not rush into a complex procedure without careful analysis of the angiogram and planning for the procedure