Background:Constrictive pericarditis is a rare but severe late complication following cardiac surgery. In our case, extensive pericardial calcification caused not only restrictive ventricular filling but also mechanical compression due to fixation of the epicardial coronary arteries, resulting in angina pectoris symptoms.
Case Presentation:A 58-year-old male, who had undergone patch closure of a primum-type atrial septal defect at the age of seven, presented with progressive exertional dyspnea and recent onset of typical effort-related angina pectoris. He was in good general condition (height 178cm, weight 71kg).
Electrocardiography showed chronic atrial fibrillation with a left bundle branch block. Transthoracic echocardiography demonstrated preserved left ventricular systolic function but markedly impaired myocardial deformation in the lateral wall, demonstrated by strain imaging (Fig.1a). Also we saw a massive left atrial enlargement (188 mL/m²) with reduced systolic strain (4.7%), and a respiratory variation of mitral inflow suggestive of pericardial constriction. Moderate mitral regurgitation due to severe annular and valve calcification was also observed.
Cardiac catheterization confirmed a typical hemodynamic pattern of constrictive pericarditis, with equalization of diastolic pressures and a dip-and-plateau configuration (end-diastolic pressure left ventricle 22 mmHg, Fig 1e). The pulmonary artery pressure was 47/20 mm Hg and cardiac output 4.1 L/min.
Coronary angiography revealed pericardial fixation of the epicardial vessels in the medial and apical segments with systolic kinking and transient obstruction of the left anterior descending artery (arrows in Fig. 1b,c,f,g). This caused a retrograde flow in the proximal vessel segments reminiscent of a bypass graft phenomenon. Similar findings were noted in the circumflex artery, explaining the patient’s angina pectoris symptoms. Heavy calcification of the mitral ring could be seen as well.
Operation and Outcome:After multidisciplinary heart team discussion, the patient underwent pericardiectomy and mechanical mitral valve replacement. Surgery was technically challenging due to massive pericardial calcification (Fig. 1d,h). Postoperative recovery under temporary circulatory support was uneventful, and the patient showed a favorable clinical outcome.
Conclusion:This case illustrates an extremely rare coexistence of constrictive pericarditis and dynamic coronary obstruction due to pericardial calcification more than five decades after primum-type atrial septal defect patch repair. The combination of exertional dyspnea and angina pectoris in such patients should prompt consideration of pericardial entrapment of coronary arteries as a contributing mechanism.
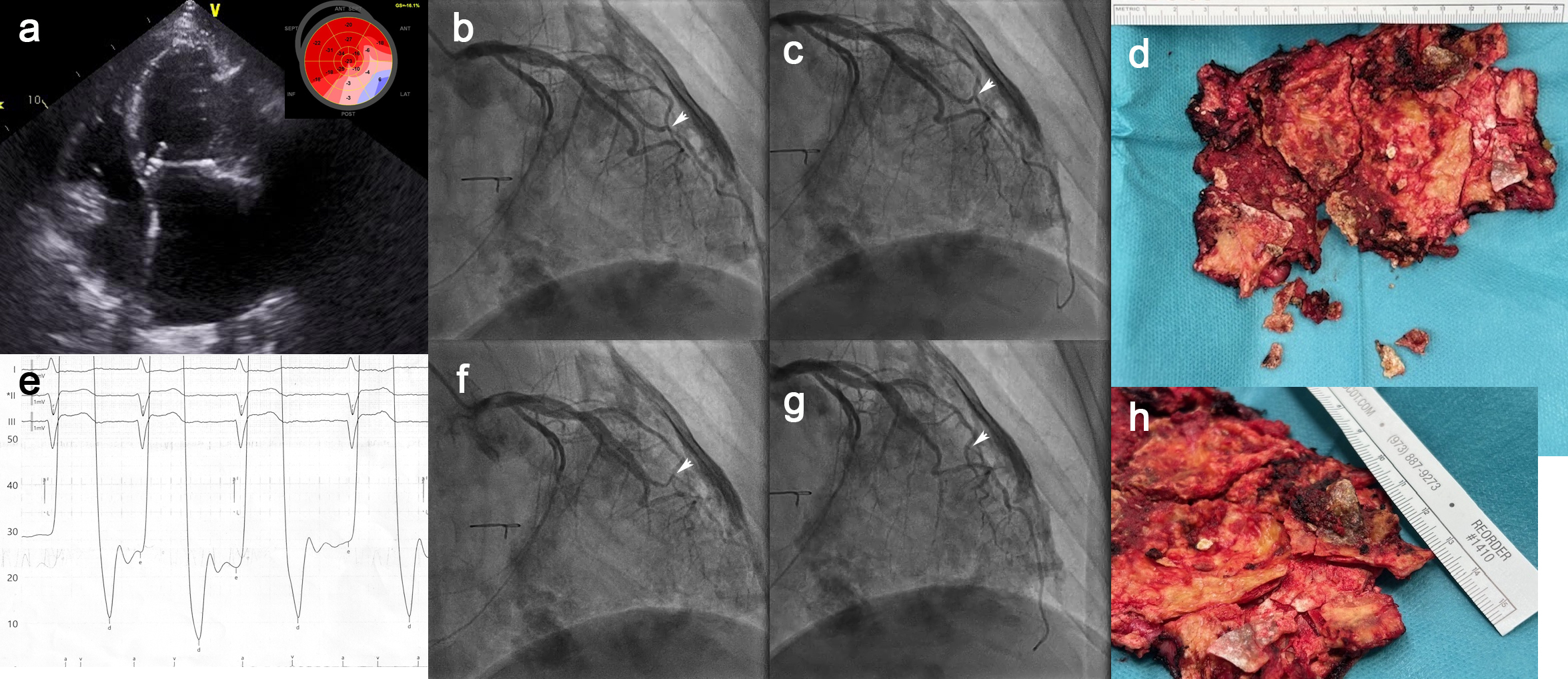
Figure 1: Constrictive pericarditis with coronary entrapment and angina pectoris five decades after surgical closure of an primum-type atrial septal defect



